All of us – no matter where we live, where we work or whether we consider ourselves left or right or somewhere in the middle – share at least one thing: We are eternally grateful for the dedication of the doctors, nurses, EMTs and other frontline responders who have worked tirelessly, even when tired-to-the-bone, throughout the pandemic.
In the early days of the COVID-19 crisis, we all remember how residents of New York City took to the streets or their balconies each night at 7 p.m. to bang on pots to show their appreciation for the work of these healthcare heroes. It was a moving sight amid so much tragedy.
But there is another group of heroes that have rarely been given the credit they deserve during these challenging times: parents.
Although children and teens sometimes forget that their parents are real people with real struggles of their own, mothers and fathers have had to deal with enormous stresses as a result of the pandemic. They’ve had to deal with social isolation, job insecurity, financial hardships, family health crises, loss of loved ones and more. Through it all, they’ve needed to be there for their kids, reassuring them that normal life would return.
Parents had an enormous amount to deal with. Young people who already dealt with various mental health issues found their symptoms heightened, while many others experienced those challenges for the first time. Depression and anxiety were (and continue to be) widespread, but many kids exhibited an increase in anger, aggressiveness and impulsivity as they attempted to manage remote schooling, the loss of social connections and activities, and the lack of privacy and space that came with 24/7 togetherness with family.
And, as kids and teens tend to do, they often took out their frustrations on their parents.
At North Shore Child & Family Guidance Center, we recognized early on that the pandemic would put a strain not only on kids but also on their families. We started a series of free, virtual Pandemic Parent Support Groups where mothers, fathers and other caregivers could express their own frustrations and learn from others that they were not alone.
With the guidance of one of our therapists, they shared ideas for helping children structure their time. They spoke of the struggles of remote schooling and learned coping strategies. They learned how to be a “container,” or a kind of safety valve, for their children’s feelings. And they were given a safe space to express their own fears.
Today, in what is often called “the new normal,” most of us are in a different place when it comes to the pandemic. Kids are back in school; the vaccine has provided a level of comfort that didn’t exist in the early days of the virus; and we are able to be out and about in the world once again, albeit with precautions and wariness.
Still, the challenges for kids and parents alike are far from over. We are just beginning to realize how the pandemic has impacted our children’s feelings of security and wellbeing, while still dealing with our own fears. Uncertainty remains about what will happen in the future.
But one thing gives me comfort: After witnessing the courage, steadfastness and love parents displayed during these last 19 months, I am certain that they will rise to the challenge.
If you are a parent or caregiver, give yourself credit for all you’ve done for your family. Be sure to engage in self-care while you continue to care for your kids and your community. The usual coping skills apply: support from friends, exercise, time in nature, meditation—whatever helps you take a deep breath and feeds your spirit.
Finally, reach out for professional support if you are feeling overwhelmed or if your children are struggling. Real heroes know that going it alone—especially as we enter the hectic holiday season—doesn’t make you brave. We are all navigating uncharted waters, and sharing our thoughts, expectations, successes and frustrations with other parents can strengthen our confidence and help steer us on a course that enhances performance, achievement and fulfilment.
Bruce Kaufstein, LCSW, is the Director of Clinical Services at North Shore Child & Family Guidance Center, Long Island’s leading children’s mental health agency, (516) 626-1971. He will be retiring from the Guidance Center at the end of this year after 37 years of dedicated service.
Childhood abuse and trauma have been serious concerns for years and, unfortunately, the pandemic seems to have exacerbated the problem. An October 2021 study presented by the American Academy of Pediatrics that analyzed 39,000 children found that 2,064 were victims of suspected child abuse during the period when pandemic restrictions were implemented, representing a significant increase from pre-pandemic. With children aged 5 and above, the average number of abuse cases nearly tripled, from 36 to 103.
Childhood trauma can be caused by a variety of circumstances, including psychological, physical or sexual abuse. It can also be caused by natural disasters, violence in the community or school, bullying, serious accidents, illnesses, loss of a loved one, stress caused by poverty, the deployment of a parent in the military, exposure to substance abuse and, in current times, fears brought on by the pandemic.
In addition, as we’ve seen in recent news reports, young people are increasingly being traumatized by school shootings, like the latest tragedy in Michigan.
Children exhibit signs of trauma in a variety of ways. Things to watch out for include:
• Anger issues • Attention problems • Changes in appetite • Development of new fears • Increased thoughts about death or safety • Irritability • Loss of interest in normal activities • Problems sleeping • Sadness • School refusal • Physical complaints such as headaches and stomachaches
Support Their Process
When helping your child deal with their emotions, it is important to remember that every person is different, and how they process their feelings will vary as well. Maryville University’s human development and family studies program highlights how impactful experiences, such as traumatic ones, can change relationships within the family and affect your child’s development. It’s during this time that they either develop trust or difficulties trusting people moving forward. Let them know that they are not alone. Always take time to listen to them when they speak about their emotions, and never trivialize them. This will ensure that they feel validated and heard.
Talk to them in situations where they feel most comfortable. This can be when you are together on a drive or having a walk through the park. Be sure to also respect their boundaries and never force them to say more than they’re comfortable sharing.
Older children and teenagers might require some time away from stresses like school pressures. As mental wellness reporter Christina Caron writes in the New York Times, allowing them to take mental health days will let them practice self-care and counter stress. Fortunately, in New York, students are allowed to take mental health days as they are treated like taking a day off due to physical illness. Supporting your child’s process will encourage their feelings of security around you.
When It’s Time for Therapy
Being there for your children does them a world of good, especially after trauma, but it’s important to acknowledge that they may need professional help during the healing process. Many parents are not properly equipped with the knowledge required to help children who have gone through traumatic events. An experienced therapist can provide your child with the right strategies and coping practices. This will also help them adjust to difficult situations without adopting unhealthy habits.
Psychology Today’s article on trauma mentions how professional psychotherapy is one of the most effective ways for those who have gone through trauma to deal with their feelings. Trauma-informed care helps build resilience and allows people to know which coping mechanisms are healthy and which aren’t.
Traumatic experiences at any age can be difficult to process, but they are even more challenging for children. Seek out help from professionals who specialize in caring for children and teens.
Note: If your child or teen is experiencing any signs of trauma, contact North Shore Child & Family Guidance Center at (516) 626-1971
When to Contact Authorities
If you suspect your child has gone through a trauma as a result of abuse or neglect, the Child Welfare Information Gateway encourages you to reach out to authorities. Signs can include reclusive behavior or bruises on the body. Bringing in the authorities may also help increase your child’s sense of safety, as they will know that the offender will no longer be able to harm them. Aside from this, it may lessen the chances of the perpetrator mistreating others in the future.
You can also call New York’s statewide number 1-800-342-3720 to make a report. Once it is filed, the central register will contact your local Child Protective Services (CPS) department and an investigation will begin within 24 hours. CPS will then determine whether or not the child is endangered within 60 days. If CPS finds evidence of abuse, the case will typically be brought to a family court. Throughout the whole ordeal, be sure that your child understands what is happening and that they feel safe. – R.J.
With Black Friday, Small Business Saturday and Cyber Monday behind us, it’s a great time to give the gift of mental health to the kids and families of Long Island!
Today is Giving Tuesday, a global celebration of generosity that provides an opportunity for people around the world to come together by sharing acts of kindness and giving their voice, time, money, goods and advocacy to support communities and causes.
Giving not only supports important causes; it also has benefits to both your physical and mental health!
A National Institutes of Health study showed that when people give back, whether through monetary donations, volunteering or other methods, it releases the “feel-good” chemicals in the brain, creating a positive feeling known as “helper’s high.” It also lowers blood pressure, leading to longer lives.
Whatever your reason for giving back, we are hoping that you show your love and concern for the young people in our community by donating today to North Shore Child & Family Guidance Center, where our mission to bring hope and healing is more important than ever before.
In the nearly two years since the pandemic struck, we’ve seen a tremendous increase in calls from schools, hospitals, ERs, pediatricians, parents and others, all reaching out for our help because the children and teens in their care are experiencing heightened levels of anxiety, depression, suicidal thoughts and other serious mental health challenges.
With your donations, we are able to make a real difference in the lives of the kids and families in our care. Here’s just a sampling of your dollars at work:
$50 covers a crisis intervention.
$85 covers one child’s group therapy session.
$125 covers one child’s individual therapy session.
$250 covers one child’s emergency assessment.
$500 covers one month of individual therapy for a child.
$1,000 covers eight therapy sessions for an entire family.
Whether you can give $10, $10,000 or somewhere in between, your generosity means the world to kids who are struggling to find help during these difficult times.
Kathy Rivera, North Shore Child & Family Guidance Center’s Executive Director/CEO, shares what she is grateful for:
“We traditionally celebrate Thanksgiving by gathering with our loved ones, ushering in the warmth and cheer of the holiday season. This year continues to bring unique challenges as no one has been spared the impact of COVID-19. Therefore, giving thanks means so much more these days.
As the Guidance Center’s new Executive Director and CEO, I am grateful for the dedication and devotion from our donors, board members and staff. Our dedicated therapists and entire team continue to perform acrobatic feats to make the holiday bright for the vulnerable families, young people, each other and the communities we serve. My family and I are grateful to celebrate another Thanksgiving holiday with one another filled with hope and laughter. Happy Thanksgiving to you all!
The Guidance Center staff is always grateful to hear from children and families that the services we provide have made a real difference in their lives. That’s especially true now, when the pandemic has created such challenging mental health issues for kids and adults alike. Here are a few comments that we’ve received from parents:
“I am writing this letter to let you know how much we have appreciated the help provided by North Shore Child & Family Guidance Center during this very difficult time. Our son was a sixth grader and was settling in very nicely until the coronavirus struck. Our therapist has been very generous with her time and has helped us navigate our way with the added anxiety created by this virus. We feel lucky to have had her guidance. Thank you for providing such a great service, and stay well.” – Mom of Middle Schooler
“I wanted to take a moment to communicate how absolutely amazing the Pandemic Parent Support Group has been. What started out as a wonderful opportunity with parents of similar-age kids turned into such a magical bonding and loving environment. My isolation and anxiety were calmed, and it gave me strength during very challenging moments. I am forever grateful!” – Pandemic Parent
“North Shore Child & Family Guidance Center can be summed up in a few words: professional, warm, committed and dedicated. I had an absolutely wonderful experience with the staff, therapist and psychiatrist as they gently bring you into the Guidance Center and nurture you all the way to the end. I really appreciate that they welcome women in all stages of motherhood from prenatal to postpartum as I had so much need for assistance during these times. In particular, my therapist was an extremely great listener; she provided invaluable insight and always had practical tools that I could use day-to-day to help deal with stressors. I can’t say enough about how amazing my experience was at the Guidance Center! Thanks so much to you all for picking me back up and helping me to thrive again.” – Maternal Depression Program Client
While Thanksgiving provides a wonderful opportunity to speak with your children and teens about the importance of being grateful, cultivating a strong sense of appreciation is something that can add value to their lives year-round. For some tips, visit our blog by clicking here.
All of us at North Shore Child & Family Guidance Center wish you a wonderful Thanksgiving!
North Shore Child & Family Guidance Center counts on donations from generous supporters like you to help us bring hope and healing to the children and families in your community. Today, our work is more important than ever before, as the mental health consequences of the pandemic have created an enormous increase of kids and teens with severe anxiety and depression. Sadly, many young people have also lost loved ones to the virus.
We know you want to do your part to make a difference! That’s why we provide so many ways to give. But at this time of year, one of the best is to consider a Qualified Charitable Distribution, also commonly known as an IRA Charitable Rollover gift.
If you are 70½ years old or older, you can take advantage of a simple way to benefit the Guidance Center and receive tax benefits in return. You can give any amount up to $100,000 per year from your IRA directly to us without increasing your taxable income.*
Here’s How it Works:
Notify your IRA custodian to make a direct transfer of the distribution amount from your IRA to North Shore Child & Family Guidance Center.
You take the portion of your required minimum distribution (RMD) that you need as income and transfer the remainder to us, thereby only paying income tax on the needed income.
Obtain a written acknowledgment from the qualified charity (different from a tax deduction receipt) to benefit from the tax-free treatment.
These are Your Benefits:
You can transfer up to $100,000 per year to charitable organizations such as the Guidance Center.
The distribution to charity counts toward your required minimum distribution for the year.
The amount transferred is excluded from your adjusted gross income.
Many taxpayers now take the standard deduction, eliminating the need for deductions associated with charitable gifts.
Here’s How to Qualify:
You must be age 70 ½ or older at the time of the gift.
Transfers must be made directly from a traditional IRA by your IRA administrator.
Gifts must be outright, and the donor cannot receive any goods or services in exchange for their contribution.
Thank you for making the wellbeing of the children and families in our community a priority as you create your philanthropic plans. We are so grateful for your support!
*Please consult your tax advisor to confirm how you would benefit from this opportunity.
Thursday is Veteran’s Day, when we honor all the brave men and women who have served our country. In addition, all of November is Military Family Appreciation Month, when families are recognized for their commitment and contributions in support of our military and nation.
Our country is facing one of the most challenging times in our history, as the pandemic continues to impact our children, who are experiencing uncertainty, anxiety and depression.
Sadly, some children are dealing with the grief of having lost parents, grandparents or other beloved family members.
For military families, these worries and losses are compounded by unique challenges. Children in these families often must deal with lengthy separations from their parents—difficult on their own, but add to that the fear that a loved one may not come home, and it’s clear why these kids are under enormous stress and experiencing heightened anxiety and depression.
Plus, military families relocate 10 times more often than civilian families—on average, every two or three years, so children face separation not only from their parents, but from their friends.
Not surprising, studies show that one third of school-age military children show behaviors such as being anxious, worrying often and crying more frequently.
Below are 20 tips from Military One Source to help military families stay strong:
TIP 1: Up your play time
Take just 15 minutes a day to play one-on-one with your child doing what he or she wants. Engaging in positive activities together reduces the need for negative discipline.
TIP 2: Speak up about your love
Let the children in your life know how much you appreciate and care for them. All children deserve to have someone who encourages them and loves them unconditionally.
TIP 3: Link up with a strong social network
Up your resilience by connecting with people who support you and make you feel good – friends, family, neighbors, religious groups, playgroups and parent groups that support families. Be sure to reach out to your installation’s Military and Family Support Center for local activities and support offerings.
TIP 4: Power up parenting. Put down the phone.
Children learn more and feel more secure when you spend unplugged, face-to-face time together. Plus, they need your attention to keep them safe. Distracted parenting is linked to an increase in injuries and accidents at home. Learn more about keeping your children safe by being actively present with them.
TIP 5: Stress up? Calm down
Too much stress makes it hard to be an effective parent. Learning how to manage stress can improve your happiness and provides a model for children to manage their own stress. Military OneSource offers stress release tips and recommended wellness apps to help cope with stress management. Reach out to your local Military and Family Support Center to find out about their available stress management classes.
TIP 6: Cuddle up to your baby
Bonding with your baby is vital. The attention you give now will last forever and help your baby grow into a healthy and happy child and adult. Check out easy ways to bond with your baby and contact your local New Parent Support Program.
TIP 7: Study up on safe sleeping
Do you know the rules for keeping a baby safe during sleep time? Babies should sleep on their backs in a safety crib and dressed in sleep clothing with no blankets or pillows. Get more information about how to create safe sleeping environments for infants.
TIP 8: Talk it up with your teen
Respect, talk and engage with your teen as much as you can. Doing things together, face-to-face time at dinner, showing affection and interest – all these can help keep teens safe and healthy. Get more ideas for positive parenting your teen. Military OneSource also offers health and wellness coaching for teens.
Powerful parenting can be learned throughout your child’s life. Pick up tips and ideas by talking to experts like counselors, doctors, teachers, family and friends. Subscribe to a good online newsletter. Read or take a class that is offered by the Family Advocacy Program. Classes are available for new or expectant military parents. You can also take advantage of Thrive, a free, online parenting-education program from the Department of Defense partnership with the Clearinghouse for Military Family Readiness at Penn State. Thrive offers evidence-based, positive-parenting practices for children from birth to age 18.
TIP 11: Pick up the right foods.
Check out the MyPlate website or the Start Simple with MyPlate app for help with healthy eating, strategies for a picky eater and ways to customize a healthy cookbook for your family. You can also explore these healthy snack tips.
TIP 12: Step up your activity.
Download the free Moving to THRIVE resource with suggestions for physical activities and play time.
TIP 13: Talk Up a Positive Parent
Compliment a father – someone you know or someone in public – on something positive you see him do with his kids. Dads contribute uniquely to children’s development (and could use the props). Moms, too!
TIP 14: Prop up another parent
A helping hand from a neighbor or friend can make a huge difference for a family under stress. Offer to babysit for the child of a friend, neighbor or family member, even if it’s just to help them rest or recharge for an hour or two. It’s also important to support a military family in the middle of a move. Check out these ways to support a MilFam before their move.
TIP 15: Thumbs up for military
Military life presents unique challenges and opportunities. Smart parents take full advantage of perks like child care, tutoring, employment support and even 24/7 counseling. Call Military OneSource at 800-342-9647 to help you get connected.
Nobody likes to think about the dangers of bullying, cyberbullying, teen dating violence, sexual assault or even child trafficking – but it can happen in any family. Learn the signs, symptoms and how to keep your teen safe.
TIP 18: Help get tots set up for deployment
Babies and toddlers can sense stress in their homes. As a caregiver, you can help them manage their strong emotions. Attend to your own emotional health as well, so you can better care for your children. Help your child prepare for deployment and explore Sesame Street for Military Families. The Talk, Listen, Connect resources are designed to help military families and their young children cope with deployments, changes and grief.
TIP 19: Listen up if your child is LGBTQ+
For youth who identify as LGBTQ+, fears of rejection are at the front of their minds. Acceptance from the family can have a positive effect, not only on a youth’s self-esteem, but also on their health and well-being. Listen, talk and learn more.
TIP 20: Step up and help a child
Strong communities strengthen families. You can help by being informed, attentive and supportive. If you are concerned about the safety or well-being of a child, help is readily available. Military OneSource has connections to reporting lines, the Family Advocacy Program and other places to turn. Find out how to report suspected child abuse.
Remember, North Shore Child & Family Guidance Center is here for your family! Call us at (516) 626-1971 for help.
Seeing grandparents walking hand in hand with their grandchildren is a heartwarming sight. But our usual assumptions about the relationship may be inaccurate. While we tend to believe that the grandparents are probably spending a few hours babysitting the kids, more and more are the primary caregivers, with their grandchildren as their full-time responsibility.
A July 2018 research update from the Butler Center for Research cites the most recent figures available from the U.S. Census, which indicate that in 2016, 2.5 million grandparents were responsible for the basic needs of one or more grandchildren under 18 years old living with them. Nearly 6 million children under 18, with 2.6 million of those under age 6, were living in their grandparents’ household.
Why the increase? Although this isn’t a new phenomenon—one prominent example is President Barack Obama, who was raised largely by his grandparents—part of the reason the figures have risen is believed to be a result of the opioid epidemic. According to the CDC, drug overdose deaths in the United States have more than tripled from 1999 to 2015, and often leave children parentless.
Other factors include incarceration, death of a parent or parents, or child abuse.
There are many concerns for these grandparent caregivers, including economic problems, as well as emotional factors, says Dr. Nellie Taylor-Walthrust, Director of the Guidance Center’s Leeds Place. “These grandparents are often isolated, struggling with health and financial issues that add additional stress to the total family,” she says.
[Source: U.S. Census Bureau]
To serve local grandparents who are in this situation, the Guidance Center created a program called C-GRASP, which stands for Caregiver Grandparent Respite and Support Program. Through C-GRASP, we provide support and education for grandparents who are the primary caregivers of their young grandchildren.
“Through partnerships with a team of supportive local entities, we provide the grandparents with a variety of services, including respite and peer support activities, counseling, clothing, food, housing assistance, transportation and school advocacy,” says Dr. Taylor-Walthrust. “Those grandparents who take part in C-GRASP feel supported by the services they receive that are designed to meet their individual needs. They also have the opportunity to develop a social network with other grandparents who are experiencing the same life challenge.”
To learn more about C-GRASP, contact the Guidance Center at (516) 626-1971.
After nearly four decades of dedicated service, our Director of Clinical Services, Bruce Kaufstein, is retiring at the end of this year, leaving behind many grateful kids, families and co-workers who have benefited from his abundant wisdom and compassion.
Kaufstein, LCSW, who interned at the Guidance Center in 1976 before joining the staff in December 1984, spent the bulk of his career working with adolescents, helping them grow and heal not only through traditional talk therapy but also with a life-changing initiative that he developed some 25 years ago: the Wilderness Respite Program, which takes at-risk adolescents on hikes and other nature activities that foster individual growth, leadership skills, self-esteem and friendships while also promoting environmental stewardship.
“Out in the natural world, in places like Bear Mountain, the teens become completely immersed and realize they have no choice but to respond to the challenges that arise, both physical and emotional,” says Kaufstein. “Sometimes they can meet those challenges independently or with a little help from the leaders, and sometimes their struggles trigger a group response to support and enable them to push on and complete the challenge of the day.”
Kaufstein, who leads the outings and is an avid hiker, explains that many of the teens have issues like autism, ADHD and anxiety, and therefore have trouble sitting still. “Out on the trails, they learn to take one step at a time to successfully complete the day’s goal,” he says. “They learn how to be independent and also how to work together. It’s so affirming for kids who rarely get much praise in school.”
He adds, “Most hikes are not characterized by struggles, but are full days of conversing, laughing, photographing nature and making friends. Since the pandemic, the value and need for interaction with peers has never been more palpable.”
Kaufstein was also the driving force behind our onsite organic gardens, where children and teens learn lessons in cooperation, responsibility and patience.“The kids take the lead in planting, watering and harvesting, and then take the produce to be donated to soup kitchens,” he explains. “It gives them an enormous sense of accomplishment and pride.”
Bruce Kaufstein speaking at our 9/11 Memorial Garden this fall.
Transforming Lives
Dr. Reena Nandi, Director of Psychiatric Services, says, “Bruce can bring calm to any situation, and he has truly transformed the lives of hundreds of children and families. He’s also been a mentor to many staff members over the years, making them feel supported and cared for. He will be sorely missed.”
Working with Guidance Center clients and their families has been a privilege, says Kaufstein, who plans to spend his retirement years hiking, playing piano and writing anecdotal stories about his experiences with adolescents. “It has been a sacred and solemn experience to positively impact the lives of so many people,” he says. “The entire staff, from the front desk people who greet clients to the senior supervisors, are so supportive of each other and of the mission. It has been incredibly gratifying to spend my career at the Guidance Center.”
Photo: Jana North, President of the UUCSR and Terry Bain, Member of UUCSR’s Board of Trustees.
When the pandemic struck in March 2020, the generous and caring members of the Unitarian Universalist Congregation at Shelter Rock (UUCSR) wanted to provide immediate financial assistance to local organizations that were impacted by the crisis.
They asked congregation members to suggest their favorite nonprofits and then set up a committee to vet the nominees. Fortunately, many UUCSR members were familiar with the lifesaving work of North Shore Child & Family Guidance Center.
After reaching out to us and hearing about our COVID-19 response efforts, UUCSR donated $10,000 to the Guidance Center and then an additional $50,000 in support of our work at a time when our services are needed more than ever. Over the course of their granting periods, UUCSR awarded $670,000 to a variety of local nonprofits to help them respond to the pandemic.
Greatest Needs
According to Terry Bain, a member of UUCSR’s Board of Trustees, the grant guidelines focused on food insecurity, homelessness, loss of parents or guardians, mental health and educational disadvantages.
“We wanted to address the areas where we thought the need would be the greatest, and in the beginning, everyone thought about food banks,” says Bain. “But by the time we got to the second round of funding, so many nonprofits were telling us about mental health issues that came out in their clients. PTSD was surfacing because the long, grinding time of the pandemic has caused such stress on everybody.”
Jana North, president of the UUCSR, says, “Of all the names that were proposed, your name rose to the top immediately. The Guidance Center is well known for doing this important work to provide services to families struggling with depression, anxiety and other issues related to COVID.”
Faith in Action
In describing UUCSR’s philanthropy efforts, North says, “We believe that with great wealth comes great responsibility. Part of what it means to be a Unitarian Universalist is to put our faith into action, and with each grant we give, we see our faith going out into the community.”
North adds that UUs “believe strongly that we are only a small part of the world around us, and our principles respect and honor the worth and dignity of each individual. We are here on this Earth only for a short time, and in that time we want to take care of each other and the planet.”
A Multifaceted Congregation
UUCSR (uucsr.org), which has about 500 members, has been holding its Sunday services virtually since the beginning of the pandemic, though some recent services have provided an onsite, outdoor option.
The congregation is a very active one, with a variety of programs, committees and events, some open to the public. For example, on the second Friday night of each month, UUCSR presents “Soulful Sundown,” a musical collaboration between Rev. Jennifer L. Brower and the Cosmic Orchestra, often with special guest musicians.
Of its many opportunities for involvement, UUCSR features a Women’s Group, Social Justice Group, Green Sanctuary Committee and LGBTQ+ Group, among others. Activities range from yoga and quilting to book discussions and bridge.
“Unitarian Universalists believe in offering respect and dignity to everyone and this includes those in a mental health crisis situation,” says Rev. Dr. Natalie Fenimore, Lead Minister. “The congregation has long sought to support mental health, spiritual health, well-being and healing.”
In fact, the UUCSR Mental Health group holds programs and discussions to broaden general awareness and increase the understanding of mental health issues and sponsors a mental health support group which met at the congregation pre-pandemic. Additionally, the congregation has provided funding for training the police in mental health crisis intervention.
Valued Partners
Kathy Rivera, the Guidance Center’s Executive Director, says, “We are so grateful to the members of UUCSR for choosing us as a grantee. Their awareness of the importance of the mental health of our children and families during the pandemic is clear evidence of their dedication to the community, and we are proud to call them one of our valued donors and partners.”
Bain of UUCSR’s board says, “It’s very challenging for parents to know where to turn for help. The fact that the Guidance Center is out there helping people is just remarkable and so needed.”
To learn more about supporting North Shore Child & Family Guidance Center, contact Director of Development Lauren McGowan at (516) 626-1971, ext. 320.
From SAMHSA, the Substance and Mental Health Services Administration
For many parents having their child return to school feels more significant this fall, with many schools opening for in-person learning following COVID-19 related closures or disruptions over the past 18 months. And while schools adapted to bring students back into the school building, parents and students had to navigate the challenges and emotions that accompany this transition.
As a parent, you may still be helping your child to process their feelings and concerns as they adjust to being back in school. By keeping the lines of communication open and giving them a safe space to share how they feel and ask any questions they may have, you will give your child the support they need to adjust to their new routine and thrive in the school environment throughout the year. SAMHSA has resources available to help parents, teachers, and schools navigate the transition back to the classroom.
Regular and open conversations with your child are beneficial any time of year and are an opportunity to address a variety of important issues. The month of October is recognized as National Youth Substance Use Prevention Monthand is an opportunity to join a broader effort to reduce substance use among our Nation’s youth. As a parent you can make a real difference by talking with your child about these issues and keeping the lines of communication open for continued conversations. Although it may not always seem like it, children do hear the concerns of their parents and other adult role models, which is why it’s so important to discuss early and often the risks of using alcohol and other drugs.
SAMHSA’s “Talk. They Hear You.” campaign recently launched a new mobile app that helps parents and caregivers prepare for some of the most important conversations they may ever have with their kids- conversations about alcohol and other drugs. The app shows parents and caregivers how to turn everyday situations into opportunities to talk with their children, and equips them with the necessary skills, confidence, and knowledge to start and continue these conversations as their kids get older. There is even a feature within the app where you can practice having the conversations, so you feel more comfortable when the time comes.
While alcohol and other drug use may not be your top-of-the-mind issues right now, there is no better time than this month to start having these talks with your kids. In fact, a recent NIH-funded study found that the overall rate of drug use among 10-14 year-olds remained relatively stable during the COVID-19 pandemic in 2020. The study also found that teens experiencing pandemic-related stress, depression, or anxiety, or hardship during the pandemic, were more likely to use alcohol or drugs.
The study also found that youth stress, anxiety, and depressive symptoms were all positively associated with the use of any substance, and that several pandemic-related factors increased adolescents’ likelihood of substance use. For example, youth who reported feeling “extreme” stress from the uncertainty associated with the pandemic were 2.4 times more likely to use any substance than youth who reported “very slight” stress.
It’s normal to have some anxiety of your own this time of year, and maybe you feel like you don’t always know the right thing to say to your child about alcohol and other drug use. Remember that you don’t have to do it alone! Check out these resources to help adults start—and keep up—the conversation about the dangers of drinking alcohol and using other drugs at a young age:
North Shore Child & Family Guidance Center has a great team, all of whom are dedicated to going above and beyond for each and every client. Ricardo Castillo, one of our social workers, was determined that the organic garden in our Roslyn Heights office would not be a victim of pandemic neglect.
He explains: “We use the garden to help kids learn lessons about responsibility, self-confidence, teamwork and growth. But since the pandemic hit, we have been seeing most of our clients through telehealth, so they weren’t able to be onsite to tend to the garden, and they really missed the experience. I decided to use an iPad and Zoom with them when I planted and harvested from the garden, so they could feel like they were a part of the process.”
Castillo worked on the garden through the summer and early fall, and it was a beautiful sight. “In 2020 and this year, we had a great crop of tomatoes, peppers, eggplant, strawberries and even watermelons,” says Castillo, who often dropped by on Sundays to volunteer his time.“We’re truly proud of our organic garden program, and especially grateful to Ricardo for all his work to keep the garden growing and to engage our clients in the process,” says Kathy Rivera, Guidance Center Executive Director. “Our staff always puts the needs of kids first.”
In the September 2021 column that ran in Blank Slate Media, our staff responds to parents’ concerns that their son may be suicidal.
In this monthly column, therapists from North Shore Child & Family Guidance Center answer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question: We are terribly concerned about our 16-year-old son. Although he is back in school, he has little interest in his classes, and it’s difficult to get him to go to school most days. He’s decided not to try out for the basketball team, which used to be his favorite thing in the world. He’s also stopped reaching out to his friends and become very isolated. When we’ve asked him about all of this, his answer is usually a shrug of the shoulders and some version of “What’s the point, anyhow?” We are incredibly worried and not sure what to do. – Feeling Helpless
Dear Feeling Helpless: There may be no scarier words for a parent to hear from their child than “Some days I just don’t want to go on any longer,” or a similar sentiment. The reality is that children and teens are under more stress than ever, with suicidal thinking and suicide attempts on the rise – plus, the isolation and fear surrounding the pandemic has created a dramatic increase in severe depression and anxiety.
The facts are that suicide is the second leading cause of death for ages 10-24, and more teenagers and young adults die from suicide than from cancer, heart disease, AIDS, birth defects and other diseases combined.
While the problem isn’t new, the pandemic has exacerbated it. Kids’ normal routines were upended in so many ways. They lost milestones like proms, graduations, family gatherings, sports, afterschool clubs and other activities that are important for their development. Even though many of those events have resumed, they are still living with the uncertainty that everything could change at a moment’s notice.
Here are some of the warning signs that your child or teen may be at risk of suicide:
Withdrawing from friends and family
Mood swings
Engaging in risky or self-destructive behavior
Sleeping more or less than usual
Changes in eating patterns
Increased use of drugs or alcohol
School refusal
Being depressed and crying often
Giving away possessions
Posting suicidal thoughts on the Internet
Talking about death and not being around anymore
Cutting themselves
Aggressiveness or irritability
Your first step should be talking honestly with your son about how he is feeling and communicate your concern in a loving, non-judgmental way.
Ask him directly if he has thoughts of suicide. The idea that talking about suicide will make your child more likely to act upon it is a myth. In fact, the opposite is true.
Let him know there is no shame in feeling depressed or sad and that he is not alone, especially given the unprecedented period we are experiencing.
Also ask him if he has a plan for suicide, since someone who has made a plan is at a higher risk and requires urgent attention. If the answer is yes, monitor him closely and seek immediate mental health services, either through the emergency room or an urgent mental health care facility. One option is Nassau County’s Mobile Crisis Intervention Team, 516-227-TALK.
It is very important that you consult a mental health professional for an assessment. Reassure your son that getting help is not a sign of weakness, but rather shows strength, and that despite his current state of mind, feelings don’t last forever. Allow him to give feedback on what he thinks might be helpful in his treatment.
Nassau County residents can contact us at North Shore Child & Family Guidance Center, which serves young people from birth through age 24. We promise to see urgent cases within 24 to 48 hours. If, however, you fear that he is in imminent danger, bring him to the emergency room for an immediate evaluation.
North Shore Child & Family Guidance Center’s Douglas S. Feldman Suicide Prevention Project is designed to address high-risk cases with a thorough evaluation for suicide risk, therapy and a comprehensive treatment plan. To schedule an appointment, call us at (516) 626-1971 or email intake@northshorechildguidance.org.
When COVID-19 took the life of 36-year-old Krystal Colman in April, Christina Colman, 60, of Coram, inherited a precious gift: her grandson Kacen, 2.
Colman was hospitalized with the coronavirus at the same time as her daughter, both in Stony Brook Hospital just after Easter. Krystal previously had pleurisy, an inflammation of the membranes that surround the lungs. When the elder Colman heard a “Code Blue” — which signifies a hospital emergency in a certain location — she said to her nurse, “That’s my daughter’s room.” Says Colman: “I wasn’t there when she took her last breath. I was beyond shocked.”
Colman, who works as an office assistant at Stony Brook Hospital, immediately went to court to get custody of her grandson; she plans to raise him with the help of another of her daughters, Jasmine, 31, an elementary school nurse.
“I’m not going to tell anyone that every day is peachy and sunny when you’re trying to raise a 2½-year-old,” Colman says. It’s especially challenging when mourning the loss of a daughter at the same time the child is mourning the loss of his single-parent mother. “It’s overwhelming.”
Jasmine, Christina and Kacen Colman in Coram on Aug. 3. Credit: Raychel Brightman
But through word-of-mouth, Colman heard of a grandparent caregivers’ support group run by the Cornell Cooperative Extension in Riverhead. The group offers PASTA classes — it stands for Parenting the Second Time Around. The eight-week curriculum offers support to those being thrust into the new role and discusses child development, discipline and family law legal issues.
“It’s been a while since a lot of the grandparents have had 2-year-olds, 8-year-olds, teenagers in their home,” says Dinah Torres Castro, a bilingual family well-being educator for Cornell Cooperative Extension. They need to feel they can do this, she says.
HELP THROUGH PANDEMIC
Cornell also collaborates with the Amityville-based not-for-profit Hope For Youth to offer family engagement activities through a kinship caregiver grant. In August, the group resumed in-person events such as movies and field trips; a family picnic was held Aug. 30 at the Suffolk County Farm, just before Grandparents’ Day on Sept. 12. “Those things are very important when you’re going through these kinds of situations,” Colman says.Sign up for Newsday’s Family newsletter
The North Shore Child and Family Guidance Center also runs a free program called C-GRASP, Caregiver-Grandparent Respite and SupportProgram, for grandparents who are caregivers due to abandonment, substance abuse issues, incarceration or mental illness, says Nellie Taylor-Walthrust, director of the North Shore Child and Family Guidance Center’s Leed Place in Westbury. C-GRASP is run in conjunction with the Town of North Hempstead for caregiver residents 60 or older, she says.
It’s important for grandparents to see they’re not alone in what they’re doing for their families, and to be alerted to resources available to them. Grandparent caregivers often feel isolated, Taylor-Walthrust says.
“They have given up their retirement to take care of children. They don’t have a lot of social opportunities themselves.” The pandemic made their isolation and challenges worse, says Taylor-Walthrust.
“Many of them are not technologically savvy,” she says, needing guidance, for instance, with helping children to log on to their Chromebooks during at home schooling. They also initially had challenges getting food, and C-GRASP volunteers helped get supplies delivered to their doorsteps.
A CHANCE TO TALK
The hardest part for grandparent caregivers can often be financial, Torres Castro says. Extra mouths to feed, school supplies, doctors’ appointments — “it can be very costly,” Torres Castro says.
Melinda Stephenson, 45, an insurance verifier, and her husband, Dexter, 50, a care coordinator, of Hempstead are currently caring for five of their grandchildren, ages 8, 7, 5, 3, and 1 — after already raising seven children of their own. “Financially, it’s sometimes a struggle to take care of them, but we do it,” she says. She’s been able to talk to Torres Castro about such issues, she says.
The opportunity to talk to others is also valuable for Colman. “That’s not my greatest strength, talking about my daughter. When I start talking about my daughter, I turn into mush,” Colman says. Her daughter and grandson had already lived with her, so she feels Krystal’s absence even more strongly. Her grandson will often want to spend time in his mother’s former bedroom, Colman says.
Colman has done some virtual events and looked forward to meeting the other families in person with Kacen at the Aug. 30 family picnic, which she expects to help them move forward with healing.
“People need people. We’ll be able to hug each other, and if we can’t, we can at least hold hands. We’ll be able to laugh together, cry together, share together.”
Beth Whitehouse writes about families, parenting and great things to do with the kids on Long Island. She’s been a Newsday editor and shared a 1997 Newsday staff Pulitzer Prize for coverage of the crash of TWA Flight 800.
Top Photo Credit: Christina Colman, 60, of Coram, sits on the porch with her grandson Kacen, 2. Credit: Raychel Brightman
With the continuing challenges brought on by the COVID-19 pandemic, more children and teens than ever before are experiencing heightened levels of anxiety, depression and other mental health issues. North Shore Child & Family Guidance Center, which has been serving the community for nearly seven decades, is responding to the need – but to accommodate the increase, we are seeking dedicated, talented people to join our team, both in clinical roles and in office staff.
Kathy Rivera, who took on the role of Guidance Center Executive Director/CEO in June 2021 and has worked in the mental health field for more than two decades, says that the agency has “a stellar reputation” throughout the area.
“The Guidance Center is regarded as one of the premier children’s mental health organizations not only on Long Island but in the entire Tri-State/metro region,” says Rivera. “The agency is known for its highly experienced therapists who are specially trained to work with children, adolescents and their families, and also for its cutting-edge programs that have served as a model for programs across the nation.”
The Guidance Center puts values such as diversity, equity and inclusion (DEI) at the forefront, both in its therapeutic model as well as its employee culture. The staff includes bilingual, bicultural therapists and outreach workers who serve the needs of the diverse Long Island community.
In addition, the organization offers extensive benefits, including health insurance, generous paid vacation time and more.
So, if you are seeking a career in a warm, welcoming environment that encourages employee growth, please contact Kiera Cohen, Director of Human Resources, at executiveoffice@northshorechildguidance.org, or view contact information for specific positions on our careers page.
Open Positions at the Guidance Center
Here is a sampling of current job openings, both for mental health professionals and general office staff.
Child and Adolescent Psychiatrist
Substance Use Counselor
Social Work Supervisor
Clinical Social Worker
Bilingual Social Worker of Mental Health Counselor
By Christina Caron, New York Times, August 23, 2021
The decline in the mental health of children and adolescents has led to new laws allowing kids to attend to their own self-care.
By the time Ben Ballman reached his junior year in high school he was busier — and more anxious — than he had ever been.
“I had moments where it felt like the whole world was coming down on me,” he said. “It was definitely a really difficult time.”
Before the pandemic shut everything down, his day started at 6:30 a.m., when he woke up to get ready for school. Next came several Advanced Placement courses; then either soccer practice or his job at a plant nursery; studying for the SAT; and various extracurricular activities. He often didn’t start his homework until 11 p.m., and finally went to bed three hours later. Every day it was the same grueling schedule.
“It’s not even that I was going above and beyond, it was, ‘This is the bare minimum,’” said Ben, now 18 and a recent graduate of Winston Churchill High School in Montgomery County, Md. “It’s like a pressure cooker that’s locked down. There’s nowhere to escape. Eventually you just kind of burst at some point, or, hopefully, you can get through it.”
Faced with high stress levels among adolescents and a mental health crisis that includes worsening suicide rates, some states are now allowing students to declare a mental health day.
And in March, Utah decided that a “valid excuse” for a student’s absence will now include “mental or behavioral health,” broadening an earlier definition that referred to mental illness. The legislator who sponsored the bill, Representative Mike Winder, a Republican, told the television station KUTV in February that it was his daughter, then a senior at Southern Utah University, who suggested the idea.
Late last year the advocacy group Mental Health America surveyed teenagers about the top three things that would be most helpful for their mental health. More than half of the respondents cited the ability to take a mental health break or absence from either school or work. And in a Harris Poll of more than 1,500 teenagers conducted in May of last year, 78 percent of those surveyed said schools should support mental health days to allow students to prioritize their health.
Ben, the recent graduate, said that as a high school student he had spoken with classmates who were struggling and needed support but didn’t know where to turn. So he organized a coalition of students to improve mental health services for students in his state. This year he spent months supporting a mental health day bill in Maryland, but it stalled in the State Senate.
There is some debate over what constitutes a mental health day and how best to spend it. Just as there isn’t a precise definition for adults, there isn’t a consensus on what it means for children, either. Typically, it is a day to rest, recalibrate and take a break from your regular routine. Unless a state or a school district outlines specific requirements, families can interpret the term broadly.
Dr. Harold S. Koplewicz, medical director of the Child Mind Institute and a child and adolescentpsychiatrist based in New York City, views mental health days as a joyous occasion: an opportunity to have fun.
Ideally, you can use mental health days as a way to celebrate your child’s efforts in school, he said.
For example, maybe your child just finished a big project, handed it in, and the next day she said: “I’m exhausted. I want a mental health day.” In that case, taking the day off is “perfectly appropriate,” Dr. Koplewicz said.
But don’t use mental health days to help your child avoid situations at school that are making them uncomfortable, he cautioned.
Instead, try to pinpoint where that anxiety is stemming from. “Are they avoiding something because it is too challenging? Are they being hurt in some way?” he asked.
If your child doesn’t want to be in school at all or is showing symptoms of depression, like insomnia, oversleeping or a lack of interest in normal activities, take time to have a deeper conversation about what’s going on. Depending on the problem, you might need a longer-term solution rather than simply a day or two to recharge.
If your child needs time off because they are suffering from crippling anxiety or experiencing a behavioral health crisis, for example, it might not be appropriate for schools or families to label that as a “mental health day” — in fact, doing so might inadvertently minimize mental health disorders, Dr. Koplewicz said.
“Sick days are sick days, whether it’s physical or mental,” he added.
Taking a day to relax and recharge can be useful at any age, including for preschoolers, who are also susceptible to stress and exhaustion, said Jennifer Rothman, the senior manager of youth and young adult initiatives at the National Alliance on Mental Illness.
“Everyone has mental health, everyone,” she said. “Our kids are faced with so many things on a daily basis.”
And that was the case well before Covid-19. The state of children’s mental health has worsened over the last decade. Between 2009 and 2019, an increasing percentage of American youth reported feeling sad or hopeless for at least two weeks “to the degree that they could not engage in their usual activities,” the Centers for Disease Control and Prevention reported; and 70 percent of teenagers surveyed by the Pew Research Center in 2018 said anxiety and depression were major problems among their peers.
The percentage of students who seriously considered suicide or made a suicide plan has also risen in the last decade. And suicide has become the second leading cause of death among adolescents.
The pandemic has further exacerbated some of these problems. Nearly half of the parents surveyed in January by the University of Michigan’s C.S. Mott Children’s Hospital said that their teenagers had shown signs of either a new or worsening mental health condition during the pandemic. And a C.D.C. report found that the proportion of 12- to 17-year-olds visiting emergency rooms for mental health reasons rose 31 percent for most of 2020 compared with 2019.
In New York, California and Florida — homes to some of the nation’s largest school districts — there are no state laws specifying that children can take a mental health day. Legislators in each of these states have tried to change that, but those efforts have fallen flat.
In the New York City school system, which has more than 1 million students, a day off for mental or behavioral health reasons “would be treated like any other sick day,” Nathaniel Styer, a New York City Department of Education spokesman, said.
The phrase “mental health day” might make some kids and parents uncomfortable. With that in mind, the school board in Montgomery County, Md., decided that it will excuse absences taken for “student illness and well-being,” starting in the new school year.
“We didn’t want to call it a mental health day, because we know there is still stigma around that,” Karla Silvestre, the school board vice president, told Education Week in June.
Schools are also experimenting with other methods beyond mental health days to help students cope with their daily stressors. The Jordan School District in South Jordan, Utah, is using “wellness rooms,” where students can decompress for 10 minutes if they are feeling overwhelmed. And some schools in Colorado have created “oasis rooms,” a student lounge staffed with peer counselors and other resources.
Melanie Zhou, 19, who attended high school in Highlands Ranch, Colo., worked alongside other students to create the oasis rooms after a friend died by suicide.
“When my friend passed away, I had no idea how to grieve properly,” she said.
Much like Ben, Melanie felt that academics were the priority at her school, not self-care. And at home, “mental heath was not talked about very clearly or openly,” she added.
One advantage of declaring a “mental health day” and recognizing its importance at the state level is that — ideally — using this kind of language can help families start to have more open conversations about subjects related to mental health, and potentially reduce some of the stigma associated with self-care, Ms. Rothman said.
“It doesn’t necessarily mean that you have a diagnosable illness, it just means that you are taking a break,” she added.
Published originally in Anton Media, Parenting Plus column, August 20 2021, By Kathy Rivera
After working in the mental health field for more than two decades, it should have come as no shock to me when I read some of the negative responses to Simone Biles’ announcement that she was pulling out of the Olympics team competition due to anxiety and other emotional challenges—but it stung, nevertheless.
On social media, TV and other outlets, outraged commenters called her everything from a coward to a quitter to a spoiled brat. Texas deputy attorney general Aaron Reitz went so far as say that Biles was a “national embarrassment.”
Former British TV host Piers Morgan tweeted, “Are ‘mental health issues’ now the go-to excuse for any poor performance in elite sport? What a joke. Just admit you did badly, made mistakes, and will strive to do better next time. Kids need strong role models, not this nonsense.”
Would these naysayers have been so harsh if Biles had pulled out because of a broken foot or burst appendix?
These comments are a clear sign that stigma surrounding mental health issues is still pervasive. Fortunately, however, there was some very positive news: The level of support for Biles from other athletes, celebrities, public figures and everyday people far outweighed the negativity, with many describing her frankness in discussing mental health as brave and inspiring.
Olympic swimming champion Michael Phelps, who has been open about his own mental health challenges, put it this way: “We’re human beings. Nobody is perfect. It’s OK to not be OK. It’s OK to go through ups and down and emotional rollercoasters. The biggest thing is, we all need to ask for help when we go through those times.”
While few of our children are under the intense public scrutiny as are Biles, Phelps, tennis star Naomi Osaka or the many celebrities who have been discussing their mental health issues, they still face enormous pressures, especially given the disruption and fear brought on by the pandemic.
At North Shore Child & Family Guidance Center, we’ve been receiving a growing number of calls from parents concerned about their children and teens’ mental health. Many describe classic signs of depression and anxiety: withdrawal from friends, lack of interest in activities that normally gave them pleasure, mood swings, agitation, sleeplessness (or oversleeping), changes to eating patterns, substance abuse—even thoughts of suicide.
While mental health issues existed in kids long before the pandemic struck (an estimated one in five youth experience a mental illness), I believe we are on the verge of a crisis that may well surpass anything we’ve ever experienced. For many young people, their very foundations were shaken apart during the pandemic, with fear and hopelessness about the future enveloping them to the point of unending despair.
How can you help? The situation with Simone Biles has provided an opportunity for families to discuss stigma and for caregivers to teach kids that no one should ever feel ashamed if they are feeling sad, anxious or emotionally overwhelmed. You can tell your children that Simone was brave to speak out and put her mental health first. You can also let them know that you are there for them, without judgment and with an open mind and heart, whenever they are feeling down.
You can also encourage your schools, religious organizations, medical professionals and other community resources to include discussions about mental health and provide resources for kids who are having difficulties. Don’t hesitate to reach out to mental health organizations like ours for information and support.
Bottom line: It’s everyone’s responsibility to educate themselves about mental health and to stand up to stigma. Let’s use the opportunity surrounding Simone Biles’ brave decision to open up about her struggles to provide our kids with the knowledge, support and understanding they will need during the challenges that lie ahead.
Kathy Rivera, LCSW, is the new Executive Director/CEO of North Shore Child & Family Guidance Center, Long Island’s leading non-profit mental health organization which has been serving our community for nearly 70 years. The Guidance Center never turns anyone away for inability to pay. To get help for your child or to support the organization’s life-saving work, call (516) 626-1971 or visit www.northshorechildguidance.org.
Last month, family and friends of Jason Witler, a 2011 graduate of Syosset High School, gathered at the high school baseball field to celebrate the life of a young man who died this past April from an accidental overdose of a drug laced with fentanyl. The event, the Jason Daniel Witler Memorial Home Run Derby, raised funds to support the work of North Shore Child & Family Guidance Center, Long Island’s leading children’s mental health agency, which has an outpatient adolescent chemical dependency program.
Three of Jason’s closest friends—Ashley Sullo, Jordan Slavin and Max Ferro—came up with the idea of the Home Run Derby shortly after Jason’s death, explains Slavin, who had been close to Witler since kindergarten. “Several of us talked about getting together to share memories of Jason, but we realized that he would want us to do something to make people in the community happy, because he loved to make everyone laugh and smile,” Slavin said. “We also wanted to raise money for an organization that was important to Jason and his family that provides help for people struggling with addiction.”
Legislator Joshua. A Lafazan
The trio asked their Syosset High School classmate and Nassau County Legislator Josh Lafazan to help, and he was quick to join the effort, which drew more than 100 attendees. “I am overwhelmed with gratitude to all who came out to show support and participate in the Jason Daniel Witler Memorial Home Run Derby,” Lafazan said. “Working with community partners, we were able to raise thousands of dollars in Jason’s memory to support the critical work that North Shore Child & Family Guidance Center does on Long Island.”
The Journey Of Addiction According to Bonnie Witler, Jason’s mother, her son’s addiction issues began in his mid-teens. “One night, Jason came home after being out with his friends and my daughter came running into my room and said, ‘Mom, come downstairs! Jason’s barred out.’ I had no idea what she meant, but later learned it meant he was high on Xanax.”
For her part, Witler’s sister Dana had seen many friends with addiction issues, so she knew the signs when she saw them in her brother. “Addiction devastates families,” she says. “It usually starts small, with drugs like Percocet and Roxies [both opioids], but eventually they move on to cheaper and easily available drugs, even heroin, because they don’t have the money to keep up with it.”
Sadly, Witler’s addiction struggles are all too familiar for many families on Long Island and across the country. According to government reports, nationwide overdose deaths reached a record 93,000 in 2020. On Long Island, fatal drug overdoses rose 34 percent in Nassau and nearly 12 percent in Suffolk, and many experts believe the pandemic played a role in that increase.
The Witler family from left: Jordan, Dana, Bonnie and Jason (Photo courtesy of the Witler family)
Our country has been facing a worsening and deadly overdose epidemic for the past several years, and fentanyl—the drug responsible for Witler’s accidental death—is a huge factor. According to the Centers for Disease Control and Prevention, fentanyl was involved in more than 60 percent of nationwide overdose deaths last year. “Fentanyl is a powerful pain pill that’s being cut into heroin, cocaine and other drugs,” says Dr. Nellie Taylor-Walthrust, Director of the Leeds Place, North Shore Child & Family Guidance Center’s Westbury facility that houses its outpatient chemical dependency program. “It’s up to 100 times stronger than morphine, which makes it extremely cheap—and extremely deadly.”
Mental Health And Addiction Witler’s family sought help from a variety of addictions specialists during his teens. After a year-plus stretch in inpatient rehab, he returned to Syosset High School in his senior year, to the delight of his many friends. He was sober—but Bonnie Witler soon realized that her son’s issues were complicated. “As we were getting ready to shop for Jason’s senior prom, he had a meltdown,” she explained. “I took him to the emergency room, and they said he’d had a manic episode.” This was the first time anyone had suggested that Jason had a mental health condition. “I then knew that he’d been misdiagnosed most of his life,” says Witler.
Indeed, mental health challenges and addiction struggles often go hand in hand, says Taylor-Walthrust. “With the increased number of youth and adolescents seeking treatment for co-occurring disorders, the most effective outcome is to treat both disorders simultaneously,” she explained.
Witler eventually moved to Florida for treatment, and Sullo, Jason’s girlfriend from Syosset, moved down to live with him. He got a job in real estate, and his life seemed to be on the right track. “Jason was doing so well,” Sullo said. “He was clean and sober for five years, and he was dedicated to helping others stay drug-free. He was such a kind soul.”
She shares just one example: “Jason saw a guy he knew from a 12-step meeting at a gas station, and the kid didn’t look well,” Sullo recalled. “Jason made a point to get his number. For weeks, he called him every day, and they went to meetings together. He really cared about other people.”
A Mother’s Grief Turns To Activism No one is sure what happened that caused Witler’s relapse, according to his mother and friends. The pandemic isolation may have been a factor, they say, but that’s only a guess. As for Bonnie Witler, who moved to Florida a few months prior to Jason’s death to be near her son, her devastating loss has been made more bearable by her new role as an activist in the battle against addiction and the fentanyl crisis.
“I call myself a MOM, for ‘Mom on a Mission,’” Witler said, who is an active participant in various committees focusing on substance abuse, mental health and the fentanyl crisis. Witler was honored to be included in Sober House Task Force meetings created in July 2016 by Palm Beach County State Attorney General Dave Aronberg. The task force’s work has led to new regulations of sober homes and treatment centers in Florida that have become the model for other states.
Witler, who recently appeared on WSVN news channel in Florida, is also working with the head counsel of the American Medical Association to lobby congress to pass legislation related to the fentanyl crisis. “Although many drug users have heard about the dangers of fentanyl, their addiction is too strong,” Witler said, “They are playing Russian Roulette.”
She adds that, because of fentanyl, “drugs are now weapons of murder. Dealers are actually charged with homicide.” Acknowledging the widespread impact of addiction, Witler’s sister Dana said, “This is not just a Witler family problem, it’s a community problem, and that’s why sharing his story is so important. People need to realize that there’s help out there. We need to end the stigma, so people don’t think they have to handle this all alone.”
A Community Comes Together The Jason Daniel Witler Memorial Home Run Derby provided a wonderful opportunity for Jason’s friends and family to comfort each other and to honor the life of a young man who cared deeply for others. The community responded in a big way. That day, more than $8,000 was raised, but through the generosity of the incredible people who made contributions in Jason’s memory before and after the event, the total reached more than $35,000, which will support the Guidance Center’s important work.
Ken Witler, Jason’s father, was awed by the large turnout. “It was all because of the hard work of Ashley, Jordan and Max, along with Josh Lafazan and his staff.” He added, “We’re glad that the proceeds will go to the Guidance Center, knowing they will be used to help kids and families struggling with addiction issues.”
Bonnie Witler says that she was “elated” for most of the day at the memorial, as so many young people and parents approached her about how much they felt her son was a part of their family and that “they loved having him around, with his great smile and big laugh.” By the end of the day, however, the grief overcame her as she explained, “It comes in waves, and you have to feel your feelings.” But she feels best when doing all she can to prevent other families from undergoing the tremendous loss that she and her family now live with every day.
“The pain of losing a child is so enormous that some days I just don’t think I can make it,” she said. “But if I can help another life, it gives me reason to go on. Maybe Jason’s life will save hundreds of others.”
—Jenna Kern-Rugile is the Director of Communications at North Shore Child & Family Guidance Center
Helping Kids Manage Stress. Published in Blank Slate Media.
In this monthly column, therapists from North Shore Child & Family Guidance Center answer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question:When I think about my youth, it seems like it was so easy compared to what our children face today. It’s not just the pandemic—although that is certainly an enormous factor—but also the pressures from social media, school, other kids, etc. How can I help my two daughters manage all the stress that they’re facing?
– Missing the Good Old Days
Dear Good Old Days: Many adults reflect on their childhood through rose-colored glasses, remembering fun family vacations, games of flashlight tag, selling lemonade on the corner and all the other good stuff. And there’s certainly nothing wrong with reveling in such memories.
But if we take off those glasses, we’re likely to also remember the pressures of doing well in school, or the bully who made us feel frightened and small, or the fights our parents had over money.
Childhood isn’t now (and probably never was) a scene out of old sitcoms like The Andy Griffith Show or The Brady Bunch. We had plenty of stresses to manage as we grew into adulthood. Still, in modern culture, childhood stress has reached a whole new level.
As you said, the COVID pandemic is unprecedented in our lifetimes, and it not only created new and traumatic issues, it magnified the ones that already existed. While losing a normal year of school brought challenges, for many children and teens, school had been a high-pressure zone for years. Today’s youth are often overbooked with extracurricular activities. And, in the biggest change of all, they experience a constant barrage of social media messages that can often make them feel like they’ll never measure up to their peers.
One thing that is essential to healthy development is free time to daydream, but children and teens spend most of their time on digital devices, be it their smartphones, videogames or other tech gadgets.
And COVID isn’t the only worry haunting our children. Kids are not immune to the news on school shootings, climate change and social unrest, with people taking sides and forgetting how to disagree with a measure of kindness and civility.
All of these messages and non-stop activities can be overwhelming. Following are seven ways you can help your children manage their stress level and find balance in their lives.
If your kids are booked with activities and homework from dusk to dawn, ask them if they are feeling overwhelmed. Let them know you will not be disappointed if they decide to lighten their schedule.
While you can’t shield your children from your own stresses, it’s important not to overwhelm them and transfer your anxieties onto them. Be mindful of your language when discussing subjects like financial or health concerns around your kids, especially the little ones.
How you respond to stressors in your life will have a huge impact on how your children learn to do the same. Next time you are feeling overwhelmed, model behavior that can be helpful to your child, such as taking a deep breath, exercising, reading or spending time in nature.
Did your child see something on the news or hear something from friends that scared them? Don’t simply tell them not to worry; talk to them about their fears without judgment and reassure them that your family is safe.
Make sure your child is getting enough sleep. Some quick tips: Eliminate electronics at least an hour before bed; suggest that they read a book, or read with them; and when it’s time to turn off the lights, keep the room dark.
Kids feel more comfortable when the family has routines that they can depend on. One simple idea: Institute family game night, so everyone will experience a fun and relaxing time together.
If they are experiencing signs of depression and anxiety that are impacting their daily functioning, don’t be reluctant to reach out for professional help.
During the pandemic, North Shore Child & Family Guidance Center is seeing clients remotely via telehealth platforms or, when deemed necessary, in person. To make an appointment, call (516) 626-1971 or email intake@northshorechildguidance.org.
By Jonathan Haidt and Jean M. Twenge. Published in the New York Times, July 31, 2021.
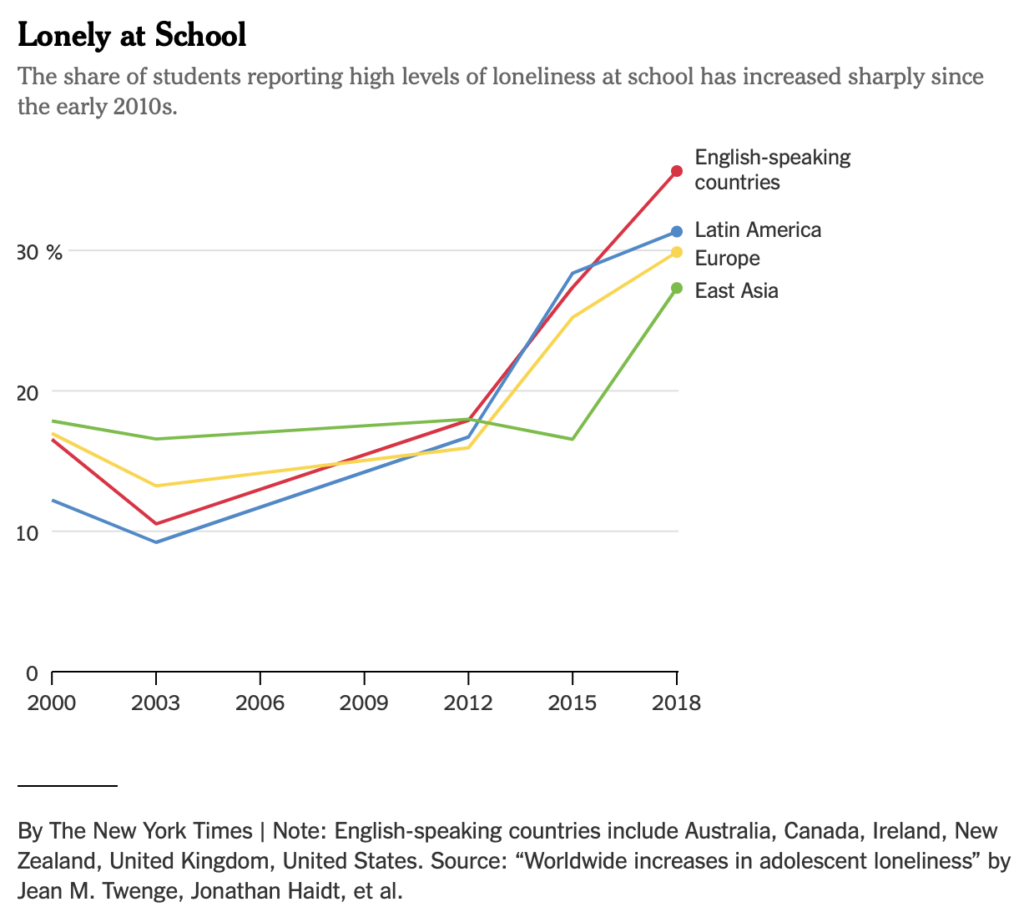
As students return to school in the coming weeks, there will be close attention to their mental health. Many problems will be attributed to the Covid pandemic, but in fact we need to look back further, to 2012.
That’s when rates of teenage depression, loneliness, self-harm and suicide began to rise sharply. By 2019, just before the pandemic, rates of depression among adolescents had nearly doubled.
When we first started to see these trends in our work as psychologists studying Gen Z (those born after 1996), we were puzzled. The U.S. economy was steadily improving over these years, so economic problems stemming from the 2008 Great Recession were not to blame. It was difficult to think of any other national event from the early 2010s that reverberated through the decade.
We both came to suspect the same culprits: smartphones in general and social media in particular. Jean discovered that 2012 was the first year that a majority of Americans owned a smartphone; by 2015, two-thirds of teens did too. This was also the period when social media use moved from optional to ubiquitousamong adolescents.
Jonathan learned, while writing an essay with the technologist Tobias Rose-Stockwell, that the major social media platforms changed profoundly from 2009 to 2012. In 2009, Facebook added the like button, Twitter added the retweet button and, over the next few years, users’ feeds became algorithmicized based on “engagement,” which mostly meant a post’s ability to trigger emotions.
By 2012, as the world now knows, the major platforms had created an outrage machine that made life online far uglier, faster, more polarized and more likely to incite performative shaming. In addition, as Instagram grew in popularity over the next decade, it had particularly strong effects on girls and young women, inviting them to “compare and despair” as they scrolled through posts from friends and strangers showing faces, bodies and lives that had been edited and re-edited until many were closer to perfection than to reality.
For many years now, some experts have been saying that smartphones and social media harm teens while others have dismissed those concerns as just another moral panic, no different from those that accompanied the arrival of video games, television and even comic books. One powerful argument made by skeptics is this: The smartphone was adopted in many countries around the world at approximately the same time, so why aren’t teens in all of these countries experiencing more mental health issues the way Americans have been? Where’s the evidence for that?
This is a difficult question to answer because there is no global survey of adolescent mental health with data before 2012 and continuing to the present. However, there is something close. The Program for International Student Assessment, or PISA, has surveyed 15-year-olds in dozens of countries every three years since 2000. In all but two administrations, the survey included six questions about loneliness at school. Loneliness is certainly not the same as depression, but the two are correlated — lonely teens are often depressed teens, and vice versa. And loneliness is painful even without depression.
So what does the PISA survey show? In a paper we just publishedin The Journal of Adolescence, we report that in 36 out of 37 countries, loneliness at school has increased since 2012. We grouped the 37 countries into four geographic and cultural regions, and we found the same pattern in all regions: Teenage loneliness was relatively stable between 2000 and 2012, with fewer than 18 percent reporting high levels of loneliness. But in the six years after 2012, rates increased dramatically. They roughly doubled in Europe, Latin America and the English-speaking countries, and rose by about 50 percent in the East Asian countries.
This synchronized global increase in teenage loneliness suggests a global cause, and the timing is right for smartphones and social media to be major contributors. But couldn’t the timing just be coincidental? To test our hypothesis, we sought data on many global trends that might have an impact on teenage loneliness, including declines in family size, changes in G.D.P., rising income inequality and increases in unemployment, as well as more smartphone access and more hours of internet use. The results were clear: Only smartphone access and internet use increased in lock step with teenage loneliness. The other factors were unrelated or inversely correlated.
These analyses don’t prove that smartphones and social media are major causes of the increase in teenage loneliness, but they do show that several other causes are less plausible. If anyone has another explanation for the global increase in loneliness at school, we’d love to hear it.
We have carried out an extensive review of the published research on social media and mental health, and we have found a major limitation: Nearly all of it, including ourown, looks for effects of consumption on the individuals doing the consuming. The most common scientific question has been: Do individual teens who consume a lot of social media have worse health outcomes than individual teens who consume little? The answer is yes, particularly for girls.
We believe, however, that this framework is inadequate because smartphones and social media don’t just affect individuals, they affect groups. The smartphone brought about a planetary rewiring of human interaction. As smartphones became common, they transformed peer relationships, family relationships and the texture of daily life for everyone — even those who don’t own a phone or don’t have an Instagram account. It’s harder to strike up a casual conversation in the cafeteria or after class when everyone is staring down at a phone. It’s harder to have a deep conversation when each party is interrupted randomly by buzzing, vibrating “notifications.” As Sherry Turkle wrote in her book “Reclaiming Conversation,” life with smartphones means “we are forever elsewhere.”
A year before the Covid-19 pandemic began, a Canadian college student sent one of us an email that illustrates how smartphones have changed social dynamics in schools. “Gen Z are an incredibly isolated group of people,” he wrote. “We have shallow friendships and superfluous romantic relationships that are mediated and governed to a large degree by social media.” He then reflected on the difficulty of talking to his peers:
There is hardly a sense of community on campus and it’s not hard to see why. Often I’ll arrive early to a lecture to find a room of 30+ students sitting together in complete silence, absorbed in their smartphones, afraid to speak and be heard by their peers. This leads to further isolation and a weakening of self-identity and confidence, something I know because I’ve experienced it.
All young mammals play, especially those that live in groups like dogs, chimpanzees and humans. All such mammals need tens of thousands of social interactions to become socially competent adults. In 2012 it was possible to believe that teens would get those interactions via their smartphones — far more of them, perhaps. But as data accumulates that teenage mental health has changed for the worse since 2012, it now appears that electronically mediated social interactions are like empty calories. Just imagine what teenagers’ health would be like today if we had taken 50 percent of the most nutritious food out of their diets in 2012 and replaced those calories with sugar.
So what can we do? We can’t turn back time to the pre-smartphone era, nor would we want to, given the many benefits of the technology. But we can take some reasonable steps to help teens get more of what they need.
One important step is to give kids a long period each day when they are not distracted by their devices: the school day. Phones may be useful for getting to and from school, but they should be locked up during the school day so students can practice the lost art of paying full attention to the people around them — including their teachers.
A second important step is to delay entry into social media, ideally keeping it entirely out of elementary and middle schools. At present, many 10- and 11-year-olds simply lie about their age to open accounts, and once that happens, other kids don’t want to be excluded, so they feel pressured to do the same.
The platforms should — at a minimum — be held legally responsible for enforcing their stated minimum age of 13. Since social media platforms have failed to do so using post-hoc detection methods, they should be required to implement age and identity verification for all new accounts, as many other industries have done. Verified users could still post under pseudonyms, and the verification could be done by reliable third parties rather than by the platforms themselves.
Even before Covid-19, teens were finding themselves increasingly lonely in school. The rapid transition to smartphone-mediated social lives around 2012 is, as we have shown, the prime suspect. Now, after nearly 18 months of social distancing, contagion fears, anxious parenting, remote schooling and increased reliance on devices, will students spontaneously put away their phones and switch back to old-fashioned in-person socializing, at least for the hours that they are together in school? We have a historic opportunity to help them do so.
Jonathan Haidt (@JonHaidt) is a social psychologist at New York University’s Stern School of Business and a co-author of “The Coddling of the American Mind.” Jean M. Twenge (@jean_twenge), a professor of psychology at San Diego State University, is the author of “iGen: Why Today’s Super-Connected Kids Are Growing Up Less Rebellious, More Tolerant, Less Happy — and Completely Unprepared for Adulthood.”
The Times is committed to publishing a diversity of letters to the editor. We’d like to hear what you think about this or any of our articles. Here are some tips. And here’s our email: letters@nytimes.com.
Recently, I spoke with a mother who was navigating an issue that has become increasingly common for many families here on Long Island and across the nation. Her 12-year-old daughter told her that she thinks she may be a lesbian, but that she’s feeling confused. The mom asked me how to best approach this conversation so her daughter would feel comfortable sharing her thoughts without fear of being judged or rejected.
The first thing I told this mom was that it’s very promising to hear that she is keeping the lines of communication open and assuring her daughter that she can trust her family to be supportive as she ponders these deeply personal questions.
More and more, we see clients at the Guidance Center who identify as part of the LGBTQ+ community; some call themselves gay or lesbian, while others are exploring their gender and/or sexual identity. Research indicates that a growing number of teenagers are identifying themselves with nontraditional gender labels such as transgender or gender-fluid, and our experience backs that up.
Regardless of the names that are used, one thing is a constant: When young people face disapproval from their families based on preferences or gender issues, they are far more likely to experience depression, anxiety, substance use and suicidal thoughts.
Research from the Centers for Disease Control and Prevention reveals the dangers of rejection. The CDC reports that LGBTQ+ youth contemplate suicide at almost three times the rate as heterosexual youth. In addition, LGBTQ+ youth who come from “highly rejecting families” are 8.4 times as likely to have attempted suicide as their LGBTQ+ peers who reported no or low levels of family rejection.
Some more eye-opening statistics: According to the Human Rights Campaign’s report, Growing Up LGBT in America, a survey of more than 10,000 LGBTQ+-identified youth ages 13-17:
4 in 10 say the community in which they live is not accepting of LGBTQ+ people.
They are twice as likely as their peers to say they have been physically assaulted, kicked or shoved.
26% say their biggest problems are not feeling accepted by their family. Other top concerns include trouble at school/bullying and fear to be out/open.
More than half (54%) say they have been verbally harassed and called names involving anti-gay slurs.
LGBTQ+ youth are more than twice as likely as non-LGBTQ+ youth to experiment with alcohol and drugs.
92% say they hear negative messages about being LGBTQ+. The top sources are school, the Internet and their peers.
Kids around the ages of 12 – 13 are at a time in their lives when they are discovering who they are, and for some, that brings up issues surrounding their sexual preferences and gender identity. As the CDC research shows, parental response is enormously important.
Youth who are exploring these issues need the unconditional support of their families, as they do with any other life concerns. They need to know they can be themselves without risking judgment.
The best response is clear: Express unconditional love and acceptance. Whether or not an adolescent ends up identifying as LGBTQ+ doesn’t change the fact that parents need to be calm and supportive. Tell them you will love them the same no matter what, and that you are there for them always.
There are some great resources to help you on this journey. One is The LGBT Network, an association of non-profit organizations working to serve the LGBTQ+ community of Long Island and Queens throughout their lifespan. It includes a group specifically for young people, called the Long Island Gay and Lesbian Youth (LIGALY), which works to build community, provide a home and safe space for all, end anti-LGBTQ+ bullying and prevent suicide. Nationally, The Trevor Project also provides lots of helpful information.
If your child or teen shows signs of depression or other mental health challenges, don’t hesitate to get help from a professional. To make an appointment at North Shore Child & Family Guidance Center, call (516) 626-1971 or email intake@northshorechildguidance.org.
Elissa Smilowitz is the Director of Triage, Emergency & Suicide Prevention at North Shore Child & Family Guidance Center, Long Island’s leading children’s mental health agency.
Gender identity terms
Gender identity: A person’s deeply held internal sense of being male or female or somewhere else on the gender spectrum.
Sex assigned at birth: The classification people are given at birth regarding sex and, typically, gender, usually based on genitalia.
Transgender: A person whose gender identity is different, and often fully opposite, from their sex assigned at birth.
Cisgender: A person whose gender identity is the same as their sex assigned at birth.
Gender nonbinary: A person who identifies as both male and female, or somewhere in between male and female.
Gender fluid: Your sense of where you are on the spectrum of male to female can change over time, even from day to day.
Sexual identity terms
Lesbian: A woman who wants to be in a relationship with another woman.
Gay: A man who wants to be in a relationship with another man (though sometimes lesbians also use this term).
Bisexual: Someone who is sexually attracted to both men and women.
Pansexual: Someone who is interested in having relationships with all genders.
If your child or teen is expressing suicidal thoughts or feelings, we can help through our Douglas S. Feldman Suicide Prevention Project. To learn more, click here.
Many people desperately want to know what to say – and what not to say – to someone who is thinking of suicide. The article 10 Things Not to Say to a Suicidal Person is SpeakingOfSuicide.com’s most popular post. Almost a half-million people have viewed it in the last 2½ years. Several hundred have left comments.
Sometimes people complain to me that the post describes what not to say, but it doesn’t say enough about what to say. They’re right. So in this post, I provide 10 things to say to a suicidal person.
First, Some Caveats
Before starting, I want to make some things clear: I came up with this list based on my conversations with suicidal individuals in my work as a clinical social worker, my readings of both clinical literature and accounts by individuals who experienced suicidal crises, and my own past experienceswith suicidal thoughts. Nobody has actually researched systematically the most effective things for friends or family to say to a suicidal person, so opinion and experience are the best we’ve got for now. Results will vary according to different people’s needs and personalities.
I also want to make clear that this list of things to say is not intended to be a script. Instead, I illustrate ways that you can help a suicidal person continue to open up, rather than shutting the person down with a comment that minimizes, invalidates, or even denigrates the person’s experience.
And I want to add that what to say often isn’t nearly as important as how to listen. As I explain in my post “How Would You Listen to a Person on the Roof?”, someone who is thinking of suicide needs to feel understood. Let the person tell their story. Refrain from immediately trying to fix the situation or make the person feel better. These efforts, however well intended, can halt the conversation.
So, with all that said, here are 10 things you can say to someone who tells you that they are considering suicide.
1. “I’m so glad you told me that you’re thinking of suicide.”
When someone discloses suicidal thoughts, some parents, partners, friends and others react with anger (“Don’t be stupid!”), pain (“How could you think of hurting me like that?”), or disbelief (“You can’t be serious.”) Some “freak out.” A suicidal person might then feel a need to comfort the hurt person, provide a defense to the angry person, or retreat internally from the disbelieving person. The person might regret ever having shared in the first place that they were thinking of suicide.
By saying “I’m glad you told me” – or something similar – you convey that you welcome and encourage disclosure of suicidal thoughts, and that you can handle it.
2. “I’m sad you’re hurting like this.”
This simple expression of empathy can go a long way toward validating the person’s pain and soothing a sense of aloneness. There’s no “Oh it’s not so bad,” no “You don’t really mean that,” no “But you have so much going for you,” no other statement denying or minimizing the person’s pain.
3. “What’s going on that makes you want to die?”
This invitation to the suicidal person to tell their story can provide validation, engender a sense of connection, and show that you really want to understand. Ask the person to tell their story. And then, listen. Really listen. To deepen your understanding, follow up with more invitations to share, like “Tell me more.” Show empathy and understanding, too: “That sounds awful” or “I can see why that’s painful.”
4. “When do you think you’ll act on your suicidal thoughts?”
Even if you’re not a mental health professional, you still can ask some basic questions to help understand the person’s risk for suicide. Asking about timing will make the difference between whether you need to call someone immediately for help (for example, if the person says, “I have a gun in my backpack and I’m going to shoot myself during lunch”) or whether you can continue to have leisurely conversation with the person.
5. “What ways do you think of killing yourself?”
This is another risk-assessment question. The answer can help reveal the gravity of the situation. A person who has put a lot of time and thought into suicide methods might be in more danger than someone with a vague wish to be dead, for example.
Understanding the suicide methods that the person has considered also will help you in your efforts to keep the person safe. For example, if you’re a parent and your teenage child discloses suicidal thoughts, knowing that your teenager is considering overdosing on a painkiller alerts you to the need to lock up or throw away all potentially dangerous medications. (See this information from the Center for Youth for ways to make your home safer.)
6. “Do you have access to a gun?”
Even if you think the person doesn’t own a gun or can’t get a hold of one, this information is always important. If the answer is yes, ask the person to consider giving the gun (or a key piece of the gun) to someone, locking the gun up and giving someone the key, or doing something else to make the home gun-free until the danger of suicide goes down. For more information about firearm safety related to suicide risk, also see this gun safety fact sheet.
Definitely tell the person about resources for help, but also make clear that you are available, too, if you’re able to do so. That said, there’s only so much you can do, so if you are feeling solely responsible for keeping the person alive, it’s best to involve others, too.
9. “I care about you, and I would be so sad if you died by suicide.”
Be careful here. In my earlier post, one of the 10 things not to say is, “Don’t you know I would be devastated if you killed yourself? How could you think of hurting me like that?” As I note in that post, “Your loved one already feels awful. Heaping guilt on top of that is not going to help them feel soothed, understood, or welcome to tell you more.”
At the same time, a simple statement of how much you care about or love the person can help nurture a sense of connection, if your statement isn’t an attempt to stop the person from talking further about suicide.
10. “I hope you’ll keep talking to me about your thoughts of suicide.”
Just as you want the person to feel welcome for having shared their suicidal thoughts to you, it’s good to make clear that you would welcome further disclosures, as well. Often, someone who has suicidal thoughts senses from others an expectation to “get over it already.” By inviting the person to come to you again about their suicidal thoughts, you can help prevent isolation and secrecy.
What Are Your Ideas about What to Say to a Suicidal Person?
There are many other helpful responses besides those listed here. If you have thoughts of suicide, what do you wish someone would say to you if you told them? If you have ever helped a suicidal friend or family member, what responses from you seemed to foster sharing, connection, and safety? Please feel free to leave a comment below.
If your child or teen is expressing suicidal thoughts or feelings, we can help through our Douglas S. Feldman Suicide Prevention Project. To learn more, click here.
In this monthly column, therapists from North Shore Child & Family Guidance Centeranswer your questions on issues related to parenting, mental health and children’s well-being. To submit a question, email communications@northshorechildguidance.org.
Question: Our grandson’s pediatrician recently suggested his parents get him screened for autism. We’re so worried and not sure where to turn. Help!
Panicked Grandparents
Dear Panicked Grandparents: There are a wide range of autism spectrum disorders, also known as ASD, and many people with the condition live very happy lives. Your first step: Get educated.
Most babies start to show an interest in the world and the people around them at a very young age. By their first birthday, typical toddlers look people in the eye, copy words, play games like peek-a-boo and engage in clapping, waving hello and good-bye and other simple behaviors.
According to the Centers for Disease Control and Prevention, people with ASD—which is a complex developmental disability that manifests in many different ways and to many different degrees—may struggle with social, emotional and communication skills.
Children or adults with ASD might…
show no interest in objects (for example, not point at an airplane flying over)
avoid eye contact
prefer not to be held or cuddled
appear to be unaware when people talk to them, but respond to other sounds
repeat or echo words or phrases said to them
have trouble expressing their needs using typical words or motions
have trouble adapting to changes in routine.
Other signs include a child not responding to his or her name when called; repeating actions over and over; and having highly restricted interests.
Early intervention is important, but even with older children, treatment can result in real improvements. At North Shore Child & Family Guidance Center, we provide thorough testing and, depending on the results, will create a customized therapeutic treatment plan, which often includes social skills groups and play therapy.
Support groups for caregivers are also very helpful. In addition to parent support groups, we have a program called GASAK, which stands for Grandparent Advocates Supporting Autistic Kids.
Also, our staff includes family advocates who often get involved in the cases, helping clients get appropriate services from their schools and other providers.
The bottom line: It’s important to determine the child’s needs and come up with a good educational and therapeutic plan. Although people with ASD may face challenges, a diagnosis doesn’t mean your grandchild won’t experience feelings of love, bonding and joy. The child is still the same loving child they were before the diagnosis. It’s a condition they have, but it doesn’t have to define their life.
Question: Now that it’s safe to be with their friends, how can I convince my kids to put their phones and tech devices down?
Sick on the Screens
Dear Sick of the Screens: During the height of the pandemic, many families made allowances for extra time on screens and now face resistance to reestablishing more strict limits.
No parent wants technology to rule the roost, especially if it’s making your children isolated. Remember, you have the power!
Set aside specific times at home when no one (parents included) uses technology. Cell phones, computers, iPads—all must be off. Tech-free time can be spent reading, talking, playing games, cooking, making art… anything creative or social will do.
Establish a clear schedule. When it comes to gaming, many parents may allow 30 minutes a day during the school week and two hours a day on the weekends.
When possible, keep all technology in a common space like the living room — not in a child’s bedroom. Avoid allowing your kid to disappear for hours behind a closed door.
Utilize online services that filter out inappropriate or violent material. These services can also limit Internet access by scheduling times that the Internet is available and times when it is not.
The way you use tech devices influences your ability to effectively guide your children. Although your example is not the sole factor, keep in mind that as distant as some kids become from adults as they are moving through their teen years, they continue to observe you—more closely than you know.
During the pandemic, North Shore Child & Family Guidance Center is seeing clients remotely via telehealth platforms or, when deemed necessary, in person. To make an appointment, call (516) 626-1971 or email intake@northshorechildguidance.org.
When Marie, 11, called a suicide prevention hotline in October, nobody saw it coming. Not even Marie herself, who had been bottling up feelings of loneliness and sadness for months without telling anyone.
Her relationships with some of her closest friends had started to suffer when school went online last year, and she worried about losing other people in her life, too. What if they moved away? What if they died?
One weekday afternoon, she put on her headphones and listened to music while taking a walk, and she began to get increasingly upset. Even now, she isn’t sure exactly why.
“I knew that I needed help, but I didn’t really know who to go to,” she said.
She searched for a suicide prevention hotline on her phone, and wondered momentarily whether the crisis counselors would take her seriously. Then, she called.
With Marie’s permission, a counselor conferenced in Marie’s mother, Jackie, who was a 25-minute car ride away. They came up with a plan to keep Marie safe until Jackie could arrive. (Their surname and those of other families interviewed for this article are being withheld to protect their privacy. Marie is being identified by her middle name.)
The next day, Marie told her mother that “in the past, not too long before that, she had brought scissors in her bedroom with the intention of hurting herself, but didn’t know how to,” Jackie said. “I was completely blindsided.”
It wasn’t as though Jackie was unaware of the mental health crisis affecting adolescents. She works as a nurse at two different pediatric intensive care units on the East Coast, where she has treated many children who attempted suicide in the past year.
“Some of them we’ve asked, ‘How did you get the idea to do this?’” Social media is their typical response, she said. “They don’t grasp that if they hurt themselves, it might not be something we can fix, and they might not get better.”
Interviews with mental health providers and data from hospitals across the country reveal that while providers are continuing to see a surge in teenagers visiting the emergency room for mental health problems, the number of children in crisis under the age of 13 is also on the rise, and has been for years.
The youngest patient under Jackie’s care who had recently attempted suicide was 8 years old. She survived, but another child, also under 13, was not as fortunate, and became an organ donor. Jackie said that most of the children who come in after suicide attempts are girls who have overdosed on pain medication, like Tylenol. Some of them now face liver damage. Once, after a particularly difficult day at work, Jackie called her husband and asked him to lock up all the Tylenol and Motrin in their home.
“I don’t want to ever think we’re immune to these things,” she said.
‘We will see this crisis grow in the fall.’
Even before the pandemic, a mental health crisis was brewing among children struggling with bullying, abuse, eating disorders, racism or undiagnosed mental health conditions. But now, children are facing even more stressors, like the loss of a family member to Covid-19, adjusting to remote school or the anxiety of returning to in-person school.
“It’s almost like the pandemic threw gasoline on embers that were already glowing,” said Heather C. Huszti, chief psychologist at Children’s Hospital of Orange County in Orange, Calif. “We’ve never seen it this bad.”
For young children, the pain can feel endless.
“It’s like, ‘This is my life now. Do I have anything to look forward to?’” Dr. Huszti said. “Because they just can’t think long term.”
CHOC, where Dr. Huszti works, has the only inpatient psychiatric center in Orange County that can take children under 12. In order to be admitted to one of the center’s 18 beds, a child must be a current or imminent threat to themselves or to others. When the center first opened in 2018, about 10 percent of the children were under the age of 12. In 2020, that number began to increase, and now has more than doubled, Dr. Huszti said.
“We have some days where every kid in the unit is under 12,” she said.
National data shows a similar pattern. In November, the Centers for Disease Control and Prevention published a study that compared how often children came to emergency rooms in the United States for mental health reasons versus other types of concerns. The agency found that between April and October of 2020, there was a 24 percent increase in the proportion of mental health emergency department visits for kids ages 5 to 11 compared with the same period in 2019.
The problem appears to be particularly dire among girls. During 2019 and 2020, the proportion of mental health-related emergency department visits was higher for girls under 18 than it was for boys of the same age, the C.D.C. reported.
“I anticipate that we will see this crisis grow in the fall as kids return to school and are trying to adjust to making up for a year of lost development,” said Dr. Jenna Glover, a child psychologist at Children’s Hospital Colorado in Aurora.
Among children who die by suicide, there are stark racial disparities. The rate of suicide in Black children under 13 has been increasing over the last decade and is two times higher than among white children. In two editorials published on Monday in JAMA Pediatrics, the authors called on funding agencies and journals to prioritize research on Black youth suicide; and emphasized the need for preventive efforts that target stigma and institutional racism.
‘The younger the child is, the longer they wait.’
Children’s hospitals, which typically have few (if any) available inpatient beds for mental health patients, have begun to run out of room.
“The younger the child is, the longer they wait,” Dr. Huszti said. “It just breaks my heart.”
Some inpatient psychiatric units may not be able to admit kids under 12, she added, because they often require more one-on-one monitoring than older kids, as well as age-specific therapy.
In April, 11-year-old Lu and her mother, Nicole (their middle names), had to wait in an emergency room in Ohio “all day and all night” because the hospital’s 13 pediatric beds were full and two kids were in line ahead of her. They were eventually transferred to a behavioral health hospital nearby. Lu befriended other kids there who had their own mental health struggles, including some who were several years older. At one point, she saw someone get sedated and restrained.
“I was concerned,” Nicole said. “She was exposed to so much there that I wouldn’t want her to be exposed to.”
During the pandemic, Lu underwent “a really big personality change” that Nicole attributed to the “perfect storm” of isolation, hormones and genetics. (Nicole was diagnosed with depression and anxiety when she was in her early 20s.) Lu became immersed in social media, and appeared to be caught in an algorithm that kept showing her videos of sad kids, her mother said.
“I had to actually explain that to her,” Nicole said. “I was like, ‘Hey did you know if I like a picture of a pair of tennis shoes, I’m going to probably keep seeing pictures of tennis shoes?’ And she looked at me, and she was like, ‘Really?’”
A couple of months ago, Nicole had the sudden urge to check the text messages saved on her daughter’s tablet. That was when she discovered that Lu had been planning on harming herself and had also written a goodbye letter.
How did we get here?
Even though the stigma surrounding mental health care has declined somewhat in recent years, “we have not yet given people the skill set or the resources to know how to manage their mental health, how to prevent or how to respond to suicidal thoughts,” said Dr. Christine Moutier, chief medical officer of the American Foundation for Suicide Prevention.
Many children also have underlying psychological problems that simply aren’t being addressed. A study published in JAMA Pediatrics found that in 2016 half of the estimated 7.7 million children in the United States with a treatable mental health disorder did not receive treatment from a mental health professional.
Finding a provider can be difficult. The American Academy of Child and Adolescent Psychiatry reported that there is a severe shortage of child psychiatrists in nearly every state in the country. In California, for example, there are only 13 practicing child and adolescent psychiatrists for every 100,000 children under 18.
Insurance companies don’t reimburse mental health services as highly as they do medical services, which makes it far less profitable for providers to treat mental health patients, experts say. For example, in Connecticut, Medicaid reimburses hospitals $2,665 per day for a standard pediatric inpatient admission and about $1,000 per day for a pediatric psychiatric hospitalization, said Ryan Calhoun,thevice president of strategy and care integration at Connecticut Children’s.
Finally, the American Academy of Pediatrics recommends mental health screening for all children 12 and older during well-child visits, but it is not standard practice to screen children younger than that, said Dr. Tami D. Benton, psychiatrist-in-chief of child and adolescent psychiatry and behavioral sciences at Children’s Hospital of Philadelphia.
“Previously, the under-12’s were identified as a low-risk group,” she said.
That’s not the case anymore, she added.
Kate, who lives in Colorado, was in the third grade when she told her parents that she didn’t want to live anymore. For much of her childhood, she has suffered from sensory processing disorder, attention deficit hyperactivity disorder and anxiety, and she was bullied in elementary school.
“I felt like I was just a waste of space,” Kate, who is now 12, said in an interview. “I was in so much pain.”
Back when she was 8, her parents took her to the emergency room, where they stayed for about 12 hours until it was determined that Kate would be safe at home.
“You just feel like, gosh, what have I done wrong as a parent? How am I not supporting my kid?” said Hope, Kate’s mother.
“Don’t feel shame,” she advised other parents. Instead, take a deep breath and call the pediatrician or a crisis line, Hope said, “so that you don’t feel alone.”
‘There’s no place to send them.’
Connecticut Children’s hospital in Hartford does not have any inpatient beds for pediatric psychiatric patients. It takes an average of one week before kids in the emergency room can find a bed elsewhere, Dr. Jennifer Downs, the division head of child and adolescent psychiatry at Connecticut Children’s, said during an interview in late May.
On that particular day, 10 of the 37 children in the emergency room for mental health reasons were under 13. Some children wait for an inpatient bed for as long as a month, she added.
“There’s no place to send them,” said James E. Shmerling, the president and chief executive at Connecticut Children’s. “Every existing resource in the community has a backlog.”
In Colorado, the situation is also critical. This year, at any given time, about half of the kids in the pediatric emergency department at Children’s Hospital Colorado are experiencing a mental health crisis, which prompted the institution to declare a state of emergency in May.
Not only are Colorado’s emergency rooms full, so are the long-term pediatric residential facilities. More than 70 children with severe mental illness had to go out of state to find a residential treatment program over the last year and a half, some traveling as far as South Carolina, Florida or New York, said Heidi Baskfield, the vice president of population health and advocacy at Children’s Hospital Colorado. It’s a problem that other states, including Connecticut, are grappling with too.
Searching for solutions.
Health care institutions have been scrambling to find ways to treat more children with acute mental health needs. CHOC, for example, is planning to open an intensive outpatient program in the next year for children in middle school who are suicidal as well as a program to offer specialized therapy to children who are 8 and under.
At Children’s Hospital of the King’s Daughters in Virginia, there was a 300 percent increase in mental health emergency department visits among 2- to 12-year-olds from 2015 to 2020. The hospital is in the process of expanding its outpatient program to include group therapy for nearly all children, which will allow them to be treated faster than they would have if they needed to wait for one-on-one therapy, said Dr. Mary Margaret Gleason, a pediatrician and child and adolescent psychiatrist there.
“The emergency room situation is a crisis, but it will be fixed only if we look at the preventive efforts that come well before,” said Dr. Gleason, who has a special interest in working with children under 6. “When you get into the preschool age, the level of unmet needs is extraordinary.”
The hospital is also constructing a new building that will have 60 inpatient psychiatric beds — currently they have none — including units for children with neurodevelopmental disorders and kids with concurrent physical and mental health needs, for example diabetes and depression.
Connecticut Children’s is educating teachers and pediatricians about how to manage children with behavioral and mental health conditions, and provides them with a phone number for real-time advice from a mental health professional, Dr. Shmerling said. He is hoping to add a medical psychiatric unit to the hospital — with as many as 15 beds — next year.
Some states, including Colorado, are starting to funnel more money toward mental health services, though providers say even more is needed.
“For now, we do need beds to meet the surge,” Ms. Baskfield said. But, she added, children also need support from schools and at the primary care and outpatient level so that fewer of them require intensive care.
“We can’t build our way out of this crisis,” she said.If you are having thoughts of suicide, call the National Suicide Prevention Lifeline:1-800-273-8255 (TALK) or text TALK to 741741
Published originally by Johns Hopkins University, Lifelines: Stories from the Human Safety Net, 2014
A team of bilingual, bicultural social workers try to help at-risk girls
Five years ago, a 12-year-old Latina girl committed suicide in her family’s garage in the town of Westbury, NY, a diverse suburb on Long Island that has pockets of poverty and has seen an influx of immigration from Central and South American countries in the last few decades.
The town – adjacent to Old Westbury, which was cited by Forbes Magazine as the 10th most expensive zip code in the United States–is rife with overcrowded, rundown multi-family housing, and a large percentage of the population is struggling to make ends meet. Day laborers wait on corners in hopes of picking up some jobs. Many of the immigrants speak little or no English. Some are undocumented, making them hesitant to reach out for legal, medical or mental health services. Even if they are willing, they can’t apply for a driver’s license and therefore are unable to travel to appointments.
It’s an unsafe and stressful environment for anyone, but especially perilous for teenage girls.
While it’s unclear exactly what led to this particular girl’s suicide, her desperate action wasn’t an isolated event, according to Regina Barros-Rivera, Associate Executive Director at North Shore Child & Family Guidance Center, a not-for-profit children’s mental health agency whose social workers, psychiatrists, psychologists and counselors provide extensive services to residents of Nassau County, Long Island.
“We were experiencing a huge influx to our agency of Latina teens with clinical depression and suicidal thoughts,” says Barros-Rivera. “Many were failing school, exhibiting self-harming behaviors such as cutting and talking about ending their lives.”
According to the Centers for Disease Control and Prevention, (CDC), one out of every seven Latina teens attempts suicide.
Some of the girls have neurological or mental health issues, such as impulsivity connected to ADHD, Barros-Rivera notes, while others have been abused. “The girls come with different stories,” she says. “Some are suicidal because their parents are fighting all the time, and they just can’t take it anymore. Some have been sexually abused. But they all were depressed and felt that suicide was their only way out. It was a very alarming trend.”
Barros-Rivera gathered a team of bilingual and bicultural social workers and mental health counselors from North Shore Child & Family Guidance Center to review research on the topic of depression and suicide in the Latina teen population. They discovered that the trend was a nationwide problem.
Family Values
The CDC study, along with other research, indicates that the major factor contributing to the high risk of depression and suicide among first-generation Latinas is the intense pressure they’re under to adhere to the traditional values of their parents’ homeland and not become too “Americanized.”
The activities that are such an accepted part of a typical teen’s life–going to the movies, to the mall, to sleepovers–are forbidden for many Latina girls. And, if they are allowed to venture out, they’re often required to have a chaperone in the form of a parent or older brother. These unrealistic limitations make the girls feel angry, hopeless and marginalized.
In many ways, it’s not surprising that these immigrant parents are overprotective of their daughters, according to Barros-Rivera. “The families have come from very distressed lands, where they have been victims of war, violence and poverty,” she says. “Many of them have been traumatized, and they’ve come here to find safety for their children. They often hover over their daughters and watch their every move. But that leaves the girls feeling they have no way out, which creates a very dangerous situation.”
Edenny Cruz and Vilma Barber of the Guidance Center Latina Girls Project.
A Creative Solution
North Shore Child & Family Guidance Center’s high-risk team knew that something had to be done. The result: The Latina Girls Project, a multifaceted program for Hispanic girls (ages 12-16) that employs individual, family and group therapy, along with monthly outings and other activities, all designed to tackle issues such as depression, suicidal ideation, hopelessness and low self-esteem.
One of the program’s clients is Maria (not her real name), a 16-year-old with large, soulful brown eyes who was born in the United States to parents from El Salvador. According to Edenny Cruz, an LMSW who, along with Barros-Rivera, counseled Maria, the teen was severely depressed and suicidal when she began treatment. Her biggest complaint was that she hated school, and she was distraught and angry that her parents pushed her to attend.
“School wasn’t a healthy or safe place to be for me,” says Maria. “I was being bullied all the time. The other kids called me names and laughed at me ever since elementary school, and I felt like I wasn’t getting any support from the teachers.”
Maria tried to explain to her mother and father the reasons school was difficult for her, but “they didn’t understand,” she says. “They told me to ignore the bullies.” Maria’s parents thought she was being dramatic and defiant, not realizing that her behavior was a sign of depression.
The prevalence of not going to school because of safety concerns was highest among Hispanic females, at 12.6%. In comparison, white females report 7.4% and black females report 8%.
The troubled teen began to skip school, which created many heated arguments in her household. Part of the reason Maria’s parents had come to the United States was to give their children a good education–something they didn’t have in El Salvador, where they spent their days working on farms instead of studying in classrooms.
“My dad hates the fact that he can’t read or write,” says Maria. “He wants me to be more successful, so school is very important to him.”
The constant pressure and fighting at home took its toll, and Maria began to feel that suicide was her only option. “I didn’t know how to deal with everything and get rid of how I was feeling,” she says. “I felt like I was just a big bother to everyone.”
Self-Harming Behaviors
In an attempt to alleviate the pain, Maria began cutting herself–a common response to stress in teen girls.
“Some of them self harm because they feel numb,” says Barros-Rivera. “It helps them experience their pain, which paradoxically provides them with some relief. It’s also something that they are in control of, which gives them a sense of autonomy.”
According to a 2011 study, self-harm among teen girls of every nationality is common, with nearly one in 12 teens deliberately hurting themselves, most often by cutting or burning their own flesh. Self-harming is one of the strongest predictors of who will go on to commit suicide. Some of the findings:
Self-harm is common, reported by about 8 percent of 14- to 19-year-olds.
At every stage, more girls reported self-harm than boys.
Those who cut, burned or otherwise deliberately hurt themselves were more likely to be seriously depressed or anxious, and to report smoking, drinking or abusing drugs.
Similarly, a small subgroup of students who began hurting themselves as young adults were more likely to report having been depressed or anxious as teenagers. The proportion of young men and women reporting self-harm substantially declined as they aged.
For Maria, who had carefully hidden her scars, the self-injurious behavior turned out to be the impetus for her parents to get her into treatment. “I didn’t want them to know that I was cutting myself, but one day I feel asleep on the couch at home and my shirt hiked up. When my mom saw the marks on my stomach, she cried and asked what I was doing.”
Realizing the gravity of the situation, Maria’s parents took her to a psychiatrist, who put the teen on medication. According to Maria, it didn’t alleviate her depression. “I just wanted to die,” she says. “I felt like I couldn’t make my parents happy no matter what I did.”
Maria’s parents reached out to North Shore Child & Family Guidance Center and learned about the Latina Girls Project. Maria began working with Edenny Cruz, whose mother and father were born and raised in Puerto Rico. “My parents were very strict,” says Cruz, “so when Maria and the other girls talk about the conflicts with their parents, I can tell them I know just what they’re talking about.”
Fostering a Common Bond
As with many clients, Maria was resistant to counseling at first, says Cruz. “Her attitude was, if you can’t get me out of school, what good are you?” she says. “She was very angry.”
Depression in teens can look very different from depression in adults. For some depressed teens, symptoms of irritability, aggression and rage are more prominent. A depressed teenager may be hostile, grumpy, or easily lose his or her temper.
“Depression is anger turned inward,” says Barros-Rivera. “Even though the girls are angry at themselves, they might express it by behaving defiantly or becoming physically aggressive–and their mothers are the most frequent targets of their outbursts.” In other girls, depression can lead to eating or sleeping disorders, she adds. “There’s no one profile that fits all the girls.”
Cruz’s strategy to help Maria develop trust during her therapy sessions was to focus on the teen’s other interests, which included singing and cooking vegetarian food.
“Talking about their whole lives–not just their problems–is an important way to get the girls to open up,” says Cruz. “With girls who are oppositional to treatment, I tell them we can talk about whatever they like and not the things that they are sad about. Eventually, they bring up those issues on their own.”
For Maria, an important breakthrough came when the team was able to work with her district to get her into a new school that had smaller classes and psychological support systems for at-risk students. The strategy worked, and Maria’s mood improved tremendously after the placement. “The kids there are just nicer, and they understand because they all had issues with school,” she says. “We all just kind of got each other.”
Maria was grateful that the Latina Girls Project counselors had listened to her frustrations and taken action to find a school that fit her needs. “Once I liked school,” she says, “my mind wasn’t so filled with hating everything.”
Drawing from teen in Latina Girls Project
The Gender Gap
While problems such as bullying, poverty, unemployment among family members, lack of access to healthcare, and racial discrimination contribute to the teens’ depression, the cultural and gender-based expectations forced upon these girls are what create the most conflicts, according to Vilma Barber, an LCSW and member of the Latina Girls Project team.
“These girls face so many stresses that the typical American teenager doesn’t have to deal with,” says Barber. “They are expected to clean the house, cook and take care of their siblings–especially their brothers, whom they refer to as ‘the golden boys,’ ” she says. “Traditionally, boys in their culture aren’t expected to do chores, so it all falls on the girls, who are put in the role of surrogate parents.”
That was the predicament for Ana, another teen who came to the Latina Girls Project suffering from severe depression and suicidal thoughts.
Ana (a pseudonym) was born in the United States to parents from Mexico. Her father worked as a sous chef and her mother as a housekeeper; both parents were often away from home. That left the burden on her–but not her brothers.
“My brothers were treated special,” says Ana, a petite, athletic girl with thick, wavy jet-black hair. “They treated me and my sister like servants.”
“It’s very tough on the girls to be put in the position of doing everything while their brothers are given free reign,” says Barros-Rivera. “It makes them feel frustrated and insignificant.”
Ana also began her life with one huge strike against her: She was a girl–not what her father had hoped for, a fact he made crystal clear. “My dad wanted a boy,” says Ana, fighting back tears. “He told me that ever since I was little.”
According to team member Susannah Sanchez-Agosto, MA-MHC, males are valued more highly in many Hispanic families.
“The Latino culture prioritizes having a strong family unit,” she says. But that unit is highly patriarchal, with females relegated to restrictive roles. “Often you can see a mother’s care-giving for her child and submission to the father’s authority as the machista,” says Sanchez-Agosto.
The Impact of Marital Strife
In addition to bearing household responsibilities, Ana carried a lot of guilt for her parents’ failing marriage. “They fought all the time, and it was very hard,” she says. “I felt like I had to be the toughest one in the house. When my siblings and my mom were crying, I’d be the one saying, ‘Don’t cry.’ I was being the mom.”
Ana’s mother acknowledges that her daughter was under enormous pressure. “The children love their father, and our marital conflicts had a negative impact on them,” she says. But she still had a difficult time understanding why her daughter was always so irritable and sad. She compared her daughter’s life with her own impoverished childhood and felt that Ana had it easy.
“I came to the U.S. because of poverty,” says Ana’s mother, the second oldest of 12 siblings. “Many times, we would all go to sleep without having dinner.”
Those kinds of statements only made Ana feel more angry, guilt-filled and worthless. “My mom would talk about how she had to work in the fields when she was growing up and didn’t have much food to eat,” says Ana. “She’d say that my life was not nearly as hard as hers had been.”
Maria had a similar experience with her father, who blamed Maria for her problems.
“My dad would say to me, ‘I’ve given you everything, I work so hard. Why are you like this?’” she says.
When Hospitalization is Needed
All of the tensions at home led Ana to fall into a deep depression; despite being an avid reader and European history buff, she began skipping school and talking about ending her life. Her mother was so concerned that when the school called one day to say Ana had walked out, she feared that her daughter had killed herself.
“There’s a bridge by my school, and my mom thought I had jumped,” says Ana.
The school social worker recognized that Ana was in danger and recommended that she be hospitalized in an inpatient psychiatric program. Despite the difficulty of dealing with that news, Ana’s mother was grateful that the school had taken action to provide her daughter with protective care. “They made me see the seriousness of the problem,” she says.
Although Ana didn’t believe the hospital experience was helpful (“it made me feel caged in,” she says), Barros-Rivera believes that, in some cases, hospitalization is necessary.
“When it’s not clear whether the girl might act out her suicidal thoughts, the hospital is the safest place for her to be,” she says.
“They can also work to determine if she is suffering from a chemical imbalance that might be helped by medication.”
Short-term inpatient psychiatric stays increased for youth of all ethnicities but declined for older adults between 1996 and 2007, according to an August 2011 study in the Archives of General Psychiatry. Hospitalization rates increased most for children ages 5-12, going from 155 per 100,000 children in 1996 to 283 per 100,000 children in 2007. Among teens, the rate rose by about 35 percent.
But hospitalizations are typically short-term, and follow-up treatment is essential, Barros-Rivera adds. “Through the Latina Girls Project, we can help teach them how to deal with their feelings so they won’t need to go the hospital again.
Finding a Safe Place
After her release from the hospital, Ana entered the Latina Girls Project and was assigned to Vilma Barber. At first, however, both Ana and her parents were hesitant to participate in the program. “I didn’t want to come,” Ana says. “My mom cried when we came, and my dad said ‘that’s for crazy people’.”
It’s not surprising that these immigrant families are reluctant to get help, says Barros-Rivera. “Most of them had no mental health care in their countries, so it’s new to them,” she explains. “There’s a cultural taboo against seeking treatment.” Plus, for families who are undocumented, the prospect of being exposed can be frightening.
But for those who do reach out to North Shore Child & Family Guidance Center and learn about the Latina Girls Project, it quickly becomes clear that they are in a safe place. “They see that we are here to help them,” says Barros-Rivera. “And they’re so happy that we speak Spanish.”
As with most girls, it took some time for Ana to develop trust in Barber. “In the beginning, I told her that I wasn’t going to tell her anything,” says Ana.
But the teen soon realized that Barber understood her situation from personal experience, having come from a strict family in Colombia. “She knew what it was like to be in a house where the girls have to do everything and the boys are treated like princes,” says Ana. “She listened when I told her that I couldn’t do anything that my friends could do, like dating. My father didn’t even want me to look at boys.”
Latina girls client at tiki recording studio
The Desire to Fit In
According to Barber, all of the girls’ parents are suspicious of the freedoms given to the average U.S. teen; they resist acculturation, while the girls embrace it.
“The girls go to school where teens dress in a way that their immigrant parents disapprove of,” says Barber. “They want their girls to wear dresses, not jeans. It makes the girls feel like they don’t fit in.”
Dating is taboo, with parents fearing their daughters will lose their virtue, a value highly prized in their culture. “At school, the girls hear about accepting your body and your sexuality,” says Barber. “They learn about issues like homosexuality and birth control, which are things their parents don’t discuss. The only choice in their minds is abstinence.”
Candice Crawford, an LMHC who is part of the Latina Girls Project team, says that the girls aren’t only forbidden to date, they’re not even supposed to text boys. Girls who do become sexually active are a source of shame.
“I had one mother who threatened to kick her daughter out of the house and send her back to El Salvador when she found out she was having sex,” says Crawford. “She called her a slut and said she had to pay the price.”
Language and Economic Barriers
While most of the parents speak little or no English, it is the primary language spoken by the girls. When their daughters speak English at home, says Barber, “the parents often feel a sense of betrayal at the loss of their culture, which is how they perceive it.”
For the teens, their parents’ inability to communicate among the general population can be a source of embarrassment. They want their mothers and fathers to be more like their peers’ parents, many of whom come from wealthier neighborhoods.
“The Latino families are living in these pockets of poverty within middle and upper-class suburbs,” says Barber. “Our girls go to schools where kids are going skiing and doing all sorts of things they can only dream about. It’s very isolating for them.”
All of these conflicts can add up to very unhappy family relationships, says Barber, in which the parents feel abandoned by their Americanized teens while “the girls feel engulfed, trapped and overprotected.”
A Great, Big World
Recognizing the need for the girls to venture beyond their homes and neighborhoods and experience the world around them, the Latina Girls Project team brings the teens on monthly outings to a variety of cultural, natural and recreational sites. These excursions help the girls become more independent, and they also give them respite from the strict oversight and household responsibilities so common in their families.
Although Maria initially didn’t want to participate, Cruz persuaded her by leveraging the teen’s love of music and booking a group trip to see the musical Wicked–an opportunity that Maria couldn’t resist. Soon, the outings were among the teen’s favorite activities.
The outings also helped Ana overcome her resistance to participating in peer group therapy. “I felt very shy,” she says. But when she learned about the monthly trips, her attitude shifted. “They really made me want to be part of the group.”
The Mother-Daughter Relationship
In addition to the outings and the individual counseling sessions, family therapy is a key component in fostering communication and easing conflicts. While involvement by both parents is ideal, it’s the mother-daughter relationship that is most important, according to Barros-Rivera.
“The father is a part of the process, of course, and many do come to the sessions,” she says. “But for these girls, I believe that to activate long-term change, you have to tackle the mother-daughter relationship.”
A 2008 study backs up her contention. The study states, “Conflict with the mother was especially detrimental for Latina girls; highly conflictive mother-daughter relationships were associated with increased internalizing and externalizing symptomatology, and father support added little in predicting symptomatology.”
During family sessions, the therapists help the mothers learn how to let their daughters develop a sense of independence and autonomy. “We’ve found that once we work with the mothers and help them understand how to let their girls separate from them in healthy, age-appropriate ways, the whole family heals,” says Barros-Rivera, herself the daughter of strict immigrant parents from Chile. “We help them see each other’s perspectives and foster healthier communication.”
When fathers do participate in the family sessions, it often serves to help them to see their own behaviors in a new light.
“Traditionally, the parenting roles are very distinctly defined, whereby the father is the primary breadwinner and the mother the primary caregiver,” explains Sanchez-Agosto. “With family therapy, the father gains a stronger sense of his co-parenting role, becoming more involved as an emotional support.”
The goal, she adds, is to involve as many of the family members as possible. “The inclusion of the extended family is a source of strength, wisdom and influence in the nuclear Latino family.”
Regina barros-rivera and vilma barber of the Guidance Center running a group for the Latina Girls Project
The Benefits of Group Support
Peer group therapy is also an important component of the program, with parents meeting in one group and the teens meeting in another.
“In these groups, both the parents and teens are embraced and supported by those who understand their feelings,” says Barros-Rivera. “It’s such an important tool toward healing for the whole family.”
In the girls’ support group, the team helps the teens identify and practice better ways of handling their stress. The group also serves as an avenue for the girls to mature and develop mentoring skills, according to Barros-Rivera. “The ones who have begun to get better are great at engaging the new girls,” she says. “They’ve been in the same spot, and it makes them feel good about themselves when they can help others. It builds their self-esteem.”
At the parent support group, parents (mostly mothers) learn how their overprotective behavior impedes their daughters’ growth. “The mothers work hard in the group, where they’re allowed to express their fear,” says Barros-Rivera. “We discuss things like communicating with your daughter, allowing them to have friends over, and adolescent sexuality.”
In fact, says Barros-Rivera, the group suggested that Planned Parenthood be invited to speak at one of their meetings. “That was an amazing accomplishment for the program goals,” says Barros-Rivera.
Major Shifts in Family Dynamics
According to Maria, her parents’ participation in the support groups marked a major turning point; they became more understanding of her depression and let go of their self-blame, which enabled them to focus on their daughter’s needs. “They realized that I just wanted them to be there for me and listen,” says Maria. “They learned that it doesn’t help to question why I feel the way I do but to accept it and support me.”
The program has also helped many of the mothers become firmer with their sons and more understanding of their daughters’ desire to identify as American teenagers. Says Ana’s mother, “I communicate better with my daughter, and she has a chance to socialize with children who have similar problems.”
Barros-Rivera is thrilled to witness such transformations in the family dynamic. “It’s so important for the girls to get permission from their parents to move on and take advantage of the opportunities this country has to offer,” she says, adding “I love these girls.”
Moving Forward
According to Barber, once Ana saw that her mother understood her need for freedom and respite from the parental role she had taken on, the teen learned to embrace her role in the family, seeing herself less as a “parentified child” and more as a “broker,” says the counselor.
“She feels proud that she can help her siblings while their mom is at work,” says Barber. “And she no longer feels resentful about helping her mother with English translations. It makes her feel important.”
As her confidence grew, Ana – a baseball and softball fan – took a self-defense class, and she’s developed a passion for the practice. She also decided to join a school group that focuses on values such as diligence, leadership, physical fitness and responsibility.
“Ana has definitely embraced those values,” says Barber. “Having come from a family where her father told her girls aren’t strong, this is a huge shift for her.”
Although Ana’s parents are no longer together, her relationship with her father has improved significantly. He bought her a piano, and she’s been learning to play one of her favorite songs: “Don’t Stop Believing” by Journey.
Empowered and self-confident, both Ana and Maria have put their difficulties behind them and are making plans for the future. Ana hopes to leverage her athleticism and desire to help others by becoming a law enforcement official. While the teen acknowledges that her favorite television shows influenced that ambition, she says her main motivation is to help others, like her parents, who don’t have papers and are prey for unscrupulous people.
“There are so many scams out there, and it makes me so mad,” says Ana. “I want to do something to make a difference for people who can’t speak up for themselves.”
Maria is also highly motivated to reach her goals, which include going to a performing arts college and becoming a professional singer. “The program helped me to not be afraid to talk or sing in front of people,” she says. “I first sang in front of my family, and they clapped, so I felt confident enough to sing in front of my school.” She also sang at a celebration for the funders of the Latina Girls Project, bringing many of the audience to tears with her beautiful, heartfelt performance of a song called “Warrior” by her favorite singer, Demi Lovato, who was diagnosed with bipolar disorder in 2011 and has become an advocate for those with mental illnesses.
Most recently, Maria had the opportunity to record the song at a professional studio, which she calls one of the best experiences of her life. “She was so full of joy the entire time,” says Barros-Rivera, who was there for the session. “Her beautiful smile lit up the room.”
The Land of Hope and Dreams
Although their treatment has concluded, Ana and Maria, as with all graduates, are still invited on the monthly outings, which help expose them to possible career paths.
“They leave here knowing that there are options for them in this country,” says Barros-Rivera. “After we work with them in the program, they see hope; they see that there are other ways to deal with life’s challenges. They’ve developed self-reliance and self-esteem, and they no longer feel suicidal.”Barber and the entire Latina Girls Project team are incredibly proud of the progress Ana and Maria have made. “They’re very smart girls,” says Barber. “They’ve learned that it’s not a betrayal to their parents for them to want more out of life than being a caretaker for their families.”
Kathy Rivera takes on leadership role at Long Island’s leading children’s mental health organization
Roslyn Heights, NY, June 22, 2021 — North Shore Child & Family Guidance Center (the Guidance Center) is pleased to announce that today, June 22, 2021, Kathy Rivera will be the organization’s new Executive Director/CEO. Ms. Rivera is taking over the leadership role upon the retirement of Andrew Malekoff, who served the agency for 45 years.
Ms. Rivera spent the last 14 years at the Jewish Child Care Association (JCCA), where she was the Senior Vice President of Care Management Services. Her experience at this multi-service child welfare agency, which provides comprehensive social services to children and families, makes her a perfect fit for the leading role at the Guidance Center, Long Island’s leading children’s mental health organization.
“We believe Kathy will provide the strong leadership, experience and vision the Guidance Center needs to move into the future,” said Paul Vitale, Guidance Center Board President. “She has a proven track record in governance and fiscal management, and she has built and developed an expert, interdisciplinary leadership team that successfully operates a wide range of mental health, physical health, education and social well-being programs that serve more than 1,000 youth and families across Metro New York.”
“North Shore Child & Family Guidance Center’s mission not only aligns with my core values but supports my commitment to strengthening individuals and families to achieve self-determined optimum well-being,” said Ms. Rivera. “It is an honor and privilege to become part of a dynamic team and outstanding organization dedicated to ensuring equity and access with the highest quality services. I am thrilled to begin this new journey with the Guidance Center and look forward to supporting communities and families on their personal paths toward hope and healing.”
Regina Barros-Rivera will serve as COO. “The Board of Directors believes that with Kathy’s leadership and Regina’s long-standing commitment and value to the organization, the Guidance Center will continue to uphold its unwavering dedication to the Nassau community,” said Mr. Vitale.
Kathy Rivera earned her Bachelor of Arts degree from Hunter College of the City University of New York and her Master of Social Work from the Hunter College School of Social Work. She is a Licensed Clinical Social Worker and holds multiple certifications and trainings including being a Sanctuary Model (Trauma Informed) Trainer. She is a first-generation American-born child of immigrant parents from Thailand. When not working, Ms. Rivera enjoys spending leisure time with her husband, two sons and dog Luna.
About Us:
As the preeminent not-for-profit children’s mental health agency on Long Island, North Shore Child & Family Guidance Center is dedicated to restoring and strengthening the emotional well-being of children (from birth – age 24) and their families. Our highly trained staff of psychiatrists, psychologists, social workers, vocational rehabilitation counselors and other mental health professionals lead the way in diagnosis, treatment, prevention, training, parent education, research and advocacy. The Guidance Center helps children and families address issues such as depression and anxiety; developmental delays; bullying; teen pregnancy; sexual abuse; teen drug and alcohol abuse; and family crises stemming from illness, death, trauma and divorce. For more than 65 years, the Guidance Center has been a place of hope and healing, providing innovative and compassionate treatment to all who enter our doors, regardless of their ability to pay. For more information about the Guidance Center, visit www.northshorechildguidance.org or call (516) 626-1971.